
Chapter 12: Special Education and Behavior Supports
Special education is a service, not a place.
—Unknown
Opening Vignette: Calm Before the Storm
Braxton was engaged with his work completing a series of measuring tasks using classroom implements, such as measuring links, unifix cubes, and rulers. His second-grade teacher, Ms. Brown, was keeping a careful eye on Braxton and complimented him several times as he worked through measuring lines of varying sizes. When Ms. Brown turned to work with another child, however, Braxton quietly got up from his desk and walked over to the calm corner. This space had several big pillows, a fuzzy rug, and some books. The classroom had gotten louder, and it seemed like Braxton was making a productive choice.Ms. Brown continued working with another child, but some of the children facing the quiet corner started shouting, “Braxton, stop it!” Ms. Brown turned her head to see Braxton urinating on the pillows and rug in the quiet corner. She instinctively shouted, “Braxton, what are you doing?” In response, Braxton said, in a matter of fact manner, “I just wanted to do it.”
This incident was not the first time this had happened at school. Braxton also had an incident earlier in the school year during which he got frustrated and urinated on the outdoor playground equipment. Because Braxton appears calm during these incidents, other adults and his classmates believe that he is fully in control and engaging in these behaviors on purpose. When considering this behavior during a follow-up intervention meeting, it became clear that Braxton was exhibiting atypical behavior as a stress response and as a part of his diagnosis, which includes a behavioral component.
Introduction
A variety of supports can be implemented in the classroom, ranging from universal supports to intensive and individualized accommodations. Additionally, children like Braxton in the opening vignette, may benefit from a number of programs and services available in a school setting. Intensive supports and programming are provided to students because they are beneficial and equitable. Recognizing that equity, not equality, should be a guiding principle in our management structures is essential. In Figure 12.1, the need for the extra box and the ramp (so everyone has access to the game) is obvious. Striving for equity can be challenging, however, when we are implementing intensive supports, especially in the case of behavioral challenges. It is harder to know what supports are required when children have seemingly “invisible” behavioral needs. Children who have demonstrated ongoing need for behavioral support in a classroom setting, require high levels of services from a collaborative team to develop their skills and fully engage within the classroom community.
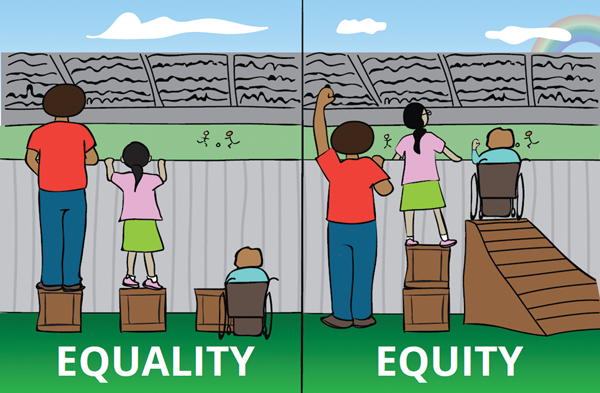
Long Description for Figure 12.1
Equality is depicted on the left side. Three people watch a sports game from behind a tall fence. One person is tall, one is shorter, and one uses a wheelchair. Each person has been given the same-sized wooden box for seeing over the fence. The tallest person stands on the box and sees everything easily. The shorter person stands on the box but still struggles to see over the fence. The person in the wheelchair is not able to use the box and can’t see the game at all. Equality gives everyone the same support, but not all benefit equally. Equity is depicted on the right side. The shorter person has two boxes and the person using a wheelchair has a ramp, so now everyone is able to see over the fence equally well.
Educators are profoundly influenced by their mental models, including implicit bias, past experiences, and current stressors (as discussed in Chapter 4). This is particularly true when considering supports that are related to behavior. As the opening vignette explores, our interpretation of a child’s behavior as noncompliant or dysregulated determines whether or not we believe the behavior to be a choice on the part of the child or the child’s internal challenges within the setting. This interpretation is value-laden and drives our response. For instance, ample evidence suggests greater numbers of Black and Hispanic children, and children from low-income environments, are identified as having disabilities, and that these disability placements are often more restrictive (Grindal et al., 2019; Kincaid & Sullivan, 2017). There is simultaneously a problem with overidentifying children as having disabilities to remedy “problem behavior” by removing them from general education spaces (Nanda, 2019); conversely, children can also be denied supports with suggestions that a child or a teacher should just try harder.
Although arduous, and sometimes overwhelming, the purpose of the special education eligibility process is designed to prevent overidentification of students who require special education, to adhere to the IDEA policy of a least restrictive environment (LRE) presented in Section. 300.114 (IDEA, 2004a), and to embrace the concept of inclusion (Francisco et al., 2020). The spirit of LRE is partially grounded in a student’s rights to a Free and Appropriate Public Education (FAPE) with the long-term vision of fostering independence to the greatest extent possible (Rehabilitation Act of 1973; U.S. Department of Education, 2010). The importance of understanding policies related to inclusion, LRE, and FAPE is to provide perspective when collaborating with larger multidisciplinary teams or navigating through special education processes.
In this chapter, we will
 discuss the classification of disabilities focused around behavioral challenges (12.1);
discuss the classification of disabilities focused around behavioral challenges (12.1); explore the people, programs, and services commonly available for addressing behavioral supports (12.2); and
explore the people, programs, and services commonly available for addressing behavioral supports (12.2); and critically examine our role as the general educator (12.3).
critically examine our role as the general educator (12.3).
12.1 Categories of Special Education
Students who present with behavioral challenges in the school setting are sometimes referred for a special education evaluation. The Individuals with Disabilities Education Act (IDEA) identified 14 separate eligibility areas for special education (IDEA, 2004b). Remember that special education eligibility is not the same as a medical diagnosis. A student may have a medical diagnosis, but may not qualify for special education services. To qualify for special education, a child must be presenting with features of a disability that significantly affect functioning in the educational setting (IDEA, 2004b).
Intervention Services for Young Children: IFSPs, IEPs, and 504 Plans
Prior to entry into the K–12 setting, early intervention services integrate education, health care, and social services. Early intervention services are provided to infants and toddlers (ages three and under) who have a disability or are exhibiting developmental delays (e.g., born premature, extended or frequent early hospitalization). In addition, a child may be considered “at risk” if there are noted adverse childhood experiences. For example, homelessness is a risk category that qualifies children for intervention services.
Early intervention is focused on developmental goals that are monitored through the process of an individualized family service plan (IFSP), which is supervised by a state appointed case manager. IFSPs must also be developed by a multidisciplinary team. The IFSP is a family-centered plan that includes services for the child and also includes services for the family (e.g., counseling). Special education and related services are also provided to children in preschool (ages three to five years old). In preschool, children may transition from an IFSP to an IEP (Smiley, Richards, & Taylor, 2022). The requirements of an IFSP are outlined in Part C of IDEA (2004d) in §303.340 and listed in Table 12.1.
| IFSPs include the following: |
|---|
|
The purpose of an individualized education plan (IEP) is to provide an appropriate education that meets the specialized needs of each student in K–12 settings. Encompassing ages 3 to 21, IEPs are sometimes present in preschool settings when services are delivered or embedded as part of the public school system and may extend beyond grade 12. IEPs are what many people think of when they refer to special education. IEP goals are focused on the educational needs of the child, and this might have a behavioral component as related to the academic setting. The team that creates an IEP includes district representatives, such as the classroom teacher, the special education teacher, parents or guardians, a person who can interpret the instructional implications of evaluation or assessment results, and, when appropriate, the student. It may also include professionals from related services (e.g., social workers, speech and language pathologists, psychologists, and occupational therapists) and may include other professionals or specialists, such as doctors. Section 300.320 (IDEA, 2004c) outlines the elements that are required in an IEP. These items are also included in Table 12.2.
| IEPs include the following: |
|---|
|
A 504 plan is the commonly used phrase for accommodations that are made under section 504 of the Rehabilitation Act of 1973 as amended, 29 U.S.C. § 794 (Section 504). These accommodations are not covered by an IEP, but instead they are put into place so that a child is able to access the educational environment to the greatest extent possible. Section 504 specifies that any entity receiving federal financial assistance cannot exclude or discriminate against a child on the basis of disability. Section 504 guarantees a free and appropriate public education to all children, regardless of the nature and severity of disability. If a child does not need specialized instruction, but does need additional supports in place, they are best served under a 504 plan.
For example, a child might have a chronic health condition that causes them to miss school on a regular basis, or miss part of the day at regular intervals. The child might miss instruction to access services such as medical or mental health care. A 504 plan could include physical accommodations, such as elevators, adapted gross motor play, removal of allergens, or use of medication at school. A 504 plan can also cover areas that cross over into behavior, such as proximity to the bathroom, a personalized schedule, headphones, or an escape pass to leave the classroom and go to the library when feeling overwhelmed.
| Medical Diagnosis or Health Condition | Possible Accommodation |
|---|---|
| ADHD | Preferential seating near the front of the classroom |
| Anxiety | Testing in small-group setting; scheduled breaks during specific aspects of the day |
| Hypotonia (low muscle tone) | Supportive seating during circle time or other events requiring children to sit on the floor |
| Asthma | Remaining indoors for recess during cold weather |
| Diabetes | Access to a certified nursing assistant for blood sugar checks, insulin administration, or more frequent snack breaks |
Special Education Disability Categories
A number of eligibility categories are difficult to assess in the early years. There are many reasons that a child might develop along their own individual trajectory that are not necessarily connected with special education eligibility. For example, a child who experiences a bout of illness for several months might experience a delay in physical, cognitive, or social emotional development because of the illness alone. A child exposed to adverse childhood experiences (ACES) might demonstrate differences in their developmental trajectory. The most common eligibility categories in young learners are early childhood developmental delay (ECDD), speech and language impairment (SLI), autism spectrum disorder (ASD), other health impairment (OHI), and emotional disturbance (ED). Each of these eligibility categories is discussed in the following sections.
Early Childhood Developmental Delay
IDEA Section 300.8 defines a child’s eligibility for special education under the category ECDD if they are “experiencing developmental delays, as defined by the State and as measured by appropriate diagnostic instruments and procedures, in one or more of the following areas: physical development, cognitive development, communication development, social or emotional development, or adaptive development” (IDEA, 2004b, B1 para. 4). Federal language allows this category to be used for children ages three through nine. Individual states may amend the age-range, by choosing to limit ECDD as an eligibility category to age seven or eight. If a child reaches the maximum age to qualify as ECDD, the multidisciplinary team first decides if the child’s education is still affected by a disability and, if so, which category best fits the child’s presentation as well as their educational needs. Although ECDD criteria seems somewhat broad and ambiguous, it is often the most appropriate category for children who are behind their peers in social and emotional development but for whom the cause of the delay cannot be attributed to a different eligibility category. With a time-limited designation and broad criteria, it allows multidisciplinary teams time and flexibility to put interventions in place and determine if a different eligibility category would best represent the child’s needs in the future.
Speech and Language Impairment
Disabilities related to speech and language are most common in early childhood settings. Many children benefit from school-based speech therapies and, most of the time, a speech delay is not comorbid with ongoing behavioral difficulties. However, there are instances in which a speech delay can negatively affect behavior. Students with receptive language delays may not process teacher or classroom directives with the same speed and comprehension of their peers, leading to a misunderstanding of rules or social skill instruction. Students with articulation difficulties or expressive language delays may become easily frustrated when their ability to communicate their needs is compromised. Children may also present with apraxia, a speech motor disorder that makes it difficult to produce some sounds or words with accuracy (Conti et al., 2020). This alone may result in periods of dysregulation that are interpreted as misbehavior in the classroom. If the maladaptive behaviors that grew out of an undeveloped ability to communicate are unintentionally reinforced when caregivers respond to the behavior rather than the original need the child tried to express, the maladaptive behavior becomes a tool or a skill that the child comes to believe is an efficient method of getting their needs met. Another component adding to a speech delay may be physiological or related to sensory needs. This is often an area that results in biting. Throughout the lifespan, humans use their mouths to explore, learn, and discharge stress. Even in adults, teeth grinding and seeking the sensory input of crunchy foods are common when an individual is experiencing stress or dysregulation (Kubo, Iinumo & Chen, 2015).
Autism Spectrum Disorder
Children who qualify for special education under the category of ASD can sometimes exhibit a range of behaviors for which additional supports are required to ensure the student’s success in a school setting. In early childhood, SLI and ASD overlap with most children qualifying as SLI before the team makes a decision to reevaluate eligibility. The behavioral challenges that may arise in children with speech delays also present themselves in children who qualify as ASD, particularly if the speech delays go beyond articulation and into apraxia. Not only does this complicate behavior if the child is frustrated, but the intent to communicate is also difficult to establish.
A reduced social drive might also appear to be a delay or impairment in language development. Communication difficulties and social deficits coincide and might also be mutually reinforcing for children with ASD (Mody & Belliveau, 2013). In addition, the frustration that comes with not being able to efficiently communicate one’s needs is compounded when a receptive language delay makes learning how to use augmentative and alternative communication difficult. Looking through a child’s lens, it is easy to see how frustration leads to ongoing behavioral issues.
Other Health Impairment
The OHI eligibility category may be considered anytime a child has a medical condition that significantly affects their ability to make progress in the general curriculum. Examples of medical diagnoses that may impact education are ADHD, seizure disorders, cerebral palsy, or psychiatric disorders. The list for which OHI eligibility may be considered is extensive, but a final determination of eligibility must be qualified by current documentation from a medical doctor or doctor of osteopathy and evidence that the disorder or disease has a negative impact on the student’s ability to make academic progress without specialized services. If these medical diagnoses are present but are not affecting academic progress, specific accommodations may be received through the implementation of a 504 plan.
Emotional Disturbance
IDEA uses the term emotional disturbance (ED) to categorize conditions, disorders, or recurrent maladaptive behaviors that manifest in the school setting and are observed for long periods of time. Individual states may use slightly different terminology like emotional impairment, emotional/behavioral disability, or emotional regulation impairment. IDEA (2004b) specifically states that the characteristics of the emotional disability must be observed over a “long period of time and to a marked degree” (34 C.F.R. 300.8 (c)(4)(i)), but it does not define what counts as a long period of time. Although taking a wait-and-see approach may be frustrating for some families and educators, it is important to be conservative in identifying school-based disabilities to avoid overidentification and placing children in educational environments that are more restrictive than necessary. Unless the behavior is part of a long-term pattern, it cannot be considered an emotional disturbance.
Closely related to ED is the diagnostic term socially maladjusted. A multidisciplinary team may, as the result of a comprehensive evaluation, determine that the student’s behavior is not related to a disability. It is often challenging to discern the difference between emotional disturbance and social maladjustment for several reasons. First, the motivation behind inappropriate behaviors depends on the observer’s perspective and societal views of behavior shift over time. Second, the two can and often do overlap. Finally, the concept of social maladjustment has not been clearly defined by IDEA with most definitions coming from case law. In the absence of a federal definition, states and local jurisdictions have latitude in their interpretation of how it intersects with emotional disturbance (Cloth et al., 2014; Nanda, 2019, Sallese et al., 2024). It is then difficult to determine which diagnosis is interfering with a child’s ability to participate in the educational system. If a child is eligible for special education services under IDEA, then they may receive supports that allow them to experience success. If, however, the behaviors are deemed to be social maladjustment, then the student is disqualified from receiving supportive services, intensive or otherwise (Cloth et al., 2014; Nanda, 2019, Sallese et al., 2024).
As a matter of ethics and equity, this approach is troublesome. There is subjectivity, and potentially bias, involved in identifying a child as defiant, impulsive, or socially aggressive. This is particularly true in a case in which identification results in a determination that services cannot help the child. This reduces difficult behaviors to a matter of virtue and willfulness on the part of the child and a matter of classroom management on the part of the teacher, while leaving out the very real need for supportive services. It also ignores what we now know about the impact of trauma on the nervous system. Just because we are not aware of potential triggers for challenging behaviors does not mean they do not exist.
Diagnoses and Behavioral Considerations
Although it is important for educators to have a basic understanding about diagnoses that impact behavior, it is equally important to remember that school systems do not assign a diagnosis for a medical or psychological disability. For instance, in some cases, students are found eligible for special education under the category of ASD, even if they have not been diagnosed with autism. Schools find children eligible under a specific set of criteria that focus on school performance and not the larger context that an outside medical diagnosis of autism entails. The reverse is true as well: Students with a medical diagnosis of autism may not qualify for a special education, if their education is not affected by the diagnosis.
There can be a tendency to jump to conclusions about diagnoses that are common in early childhood and also those that are rarely or even never diagnosed in early childhood. Making diagnostic judgments, however, is unhelpful and offers little to appropriately inform our responses. For example, fetal alcohol spectrum disorder (FASD) often results in cognitive differences, which could have an impact on behavior in areas, such as executive functioning and impulsivity. There are known distinguishing physical characteristics, but many individuals with FASD do not have distinct facial markers. Even when there appears to be facial features of FASD, assessment teams take precise measurements and look for variations in ratio that are not always apparent to the naked eye (Mattson, Bernes, & Doyle, 2019). Bipolar disorder is sometimes suggested by adults who see a child demonstrating erratic or frequent mood swings. Bipolar disorder is not a pediatric disorder, however, and it should be diagnosed only after an individual is 18 years old. Moreover, mood swings are normal and may be hormonal or situational. Children who display mood lability may be responding to toxic stress. Table 12.4 outlines myths, facts, and hard truths about diagnoses that are commonly mentioned in reference to children with behavioral difficulties.
| Myths | Facts | Hard Truths | |
|---|---|---|---|
| Autism Spectrum Disorder (ASD) | Individuals on the autism spectrum cannot make eye contact and have difficulty forming relationships. | ASD diagnostic criteria includes a wide variety of neurotypicality and abilities.Aversions to eye contact and physical touch are sometimes related to culture or one’s own experiences. | Because the spectrum is so expansive, only trained professionals have the authority to diagnose ASD, and the diagnosis is almost always a group decision by a multidisciplinary team after extensive observation, data collection, and interpretation of assessment results. |
| Attention Deficit Hyperactivity Disorder (ADHD) | Kids that cannot sit still have ADHD and kids that cannot pay attention have ADD.Kids with ADHD need medication. | ADHD has 3 subtypes: primarily hyperactive, primarily inattentive, and combined type. ADD is an outdated term.Although medication can be helpful to individuals who have been diagnosed with ADHD, introducing strategies and parental training are also effective. | ADHD shares many symptoms with complex trauma, anxiety, and FASD. Children with ADHD present in various ways across settings. Some children may need multiple layers of support to address challenging behaviors. |
| Anxiety Disorders | Shy children have anxiety.Aggressive children have anxiety.
Children who do not want to leave their parents at drop off have anxiety. |
Everyone experiences anxiety to some degree. What makes the difference between typical anxiety and a generalized anxiety disorder is the amount to which irrational anxiety affects functions of daily living in a variety of domains. | A child who is anxious at school may have good reason to be anxious: They may be experiencing bullying; they may have concerns about the home environment when they are away from it; their stress-response system may be overloaded. |
| Oppositional Defiant Disorder (ODD) | Students who demonstrate refusal behaviors have ODD.Children who are explosive during task avoidance have ODD. | ODD and many similar disorders have the same final criterion, which is that the symptoms are not better explained by something else. A clinician with the skills and authority to diagnose ODD will carefully examine and rule out other factors. | Many clinicians and psychiatrists have moved away from diagnosing ODD because of the stigma attached to it (Beltrán, Sit, & Ginsburg, 2021). In addition, behavioral presentation alone is not enough to diagnose ODD (or other disorders of behavior) because criteria fail to investigate other causes for behavior. |
12.2 People, Programs, and Services to Support
Children and families can access different types of supports when eligible for special education services. As discussed in Chapter 11, intensive intervention supports are collaborative and teachers will work with others to provide wraparound services. In this section, we explore how people, programs, and services are leveraged in different ways to meet the individualized needs of children within special education.
People
One of the most meaningful and impactful resources in any setting is people. When teachers or caregivers have concerns about how to support a child or what resources may be beneficial, they typically present their concerns to a collaborative team. These teams could be referred to as child study teams, teacher assistance teams, or intervention assistance teams. Child study teams work with families to obtain consent for additional testing and evaluation to determine special education eligibility. When a special education evaluation is initiated, a multidisciplinary evaluation team (MET) will begin to collect data relevant to the evaluation. The MET always includes parents or caregivers; the rest of the team is composed of specialists in various disciplines, depending on the nature of the suspected disabilities.
Once a child is found eligible for special education services, additional human resources are often integrated within classroom communities to meet the child’s social and emotional goals. In a school setting, a child’s primary relationship is usually with their general education teacher, but as the level of support required increases, so too do the number of support personnel. Depending on the child’s eligibility, they may also receive specialized supports from special education teachers. Other professionals that may support children with behavioral challenges are sometimes called teacher’s aides, instructional aides, or paraprofessionals. Some support personnel work in general education classrooms and some work exclusively in special education settings. Students with intense needs often have access to adult support as a condition of their IEP. Additional personnel support might look like a lower adult-to-student ratio in the general education classroom or it could mean a child receives additional support but only in specific situations like lunchtime, periods of transitions, or for specific skills like toileting or monitoring a medical condition. Further still, some children receive 1:1 paraprofessional support throughout the day, often for safety, medical care, or behavioral redirection.
Having access to an adult in the classroom to help explain instructions or context can be especially beneficial to a child who has speech delays, requires personal care, or finds interacting with peers challenging. This type of support often helps to keep a student in the general education classroom. The drawback to this level of support is that it can foster reliance rather than independence. In addition, when adult support is 1:1, it readily identifies that child as having additional needs to staff and other children, eroding a child’s right to privacy and contributing to a potentially negative stigma.
Programs
In this chapter and in the context of intensive special education resources, “program” refers to specialized classrooms. The classroom program might be within a traditional school, or it could be a separate facility. There are many benefits and limitations of specialized classroom programs. Inclusion is a key factor in decisions around special education program placement because it allows students to build authentic relationships with peers and to participate in a traditional classroom environment. It is important for programs and educators to continually monitor the value of inclusive practices and to make changes as needed.
Resource rooms, special education classrooms, and part-time classrooms are all contexts in which children receive pull-out services, often detailed in an IEP. Delivering focused instruction in a smaller group with a specialized teacher can be beneficial. If a child needs additional reading support, being pulled out during reading time can be doubly beneficial: The support is more focused and intensive, and the anxiety that comes from a lack of mastery is minimized. For students who are easily overstimulated, having access to a resource room as a “reset” may also prevent further periods of dysregulation. The greatest drawback of separate resource or special education rooms is that it removes the child from the regular classroom for part of the day. This drawback can be mitigated with strategic collaboration between the classroom teacher and the collaborating professional. In the past, a greater stigma was attached to resource rooms. Today’s school environment is more conducive to students moving between classrooms and specialists, making time in the resource room more commonplace.
Categorical or self-contained classrooms are typically set up for full-time support with a specially endorsed teacher, but students may participate on a part-time or full-time basis. Some students have needs greater than what can be provided in the general education classroom, and they benefit from a specialized classroom environment and services that are detailed in an IEP. Students with behavioral or communication needs often benefit from a specialized classroom setting while still having access to the general curriculum. The greatest benefit from categorical classrooms is that it keeps the child in their regular school building. Although the stigma that was once attached to resource rooms has fallen away, the same is not always true for self-contained classrooms. Center-based programs are special education programs that are entirely segregated from general education buildings. For a very small percentage of students, general education settings are not the least restrictive. These are situations in which the nature and severity of the student’s disability exceeds the supports available in the general setting. Some of the benefits of center-based programs include very low staff-to-child ratios, access to and space for more intensive school-based therapies, and the freedom to focus on functional skills rather than academics. One of the greatest benefits of center-based programs is the opportunity for students to develop social skills and authentic friendships with peers. The obvious limitations of center-based programs is a lack of access to the general curriculum and typically developing peers. Center-based settings are focused on supporting independence and functional skills more than particular curriculum benchmarks. When a child’s skill growth indicates that they are ready to transition back to a traditional school setting, it can be an adjustment as a child integrates into a model with decreased adult support and an increased emphasis on state or local standards.
Services
Many of the intensive resources and supports that have been discussed in this chapter can be widely referred to as supplementary services. In an IEP, a supplementary aid or service could include more basic supports like the use of headphones or a calculator. It could also include more intensive elements like access to adult support (as described earlier in this section), access to assistive technologies, or consultation with ancillary services. Supplementary services can also include a commitment to processes like the development of a behavior plan or periodic consultation with outside services. In a school setting and in the context of intensive resources, the different types of services may overlap. For example, ancillary services like speech or occupational therapy could be considered a supplementary service if the services are more consultative (supplementary) than direct. Assistive technology is also a supplementary aid, but as the development and use of technology expanded, it has grown into its own category.
Ancillary services typically refer to specialists. These roles commonly include areas such as social work, occupational or physical therapy, and speech pathology, to name a few. The obvious benefit to ancillary services is that a child is able to access therapeutic services during the school day. When these services are appropriately focused on the school setting and cannot be replicated in a clinical setting (i.e., social skills groups, in-class motor activities), they become invaluable services for a child. Although having some therapies provided in school settings is important because it is focused on educational needs, families may misunderstand the scope of these therapies and forgo outside services. Even school personnel sometimes overestimate the intensity and possibilities of school-based therapies. A child may benefit from school counseling services to facilitate group play or other social skills, but the school setting is not an appropriate setting to thoroughly address more complex issues like attachment disorders or trauma. Sometimes the opposite is true; an occupational therapist could undoubtedly assist every child in learning how to tie their shoes or properly hold a pencil, but these are developmental tasks that usually do not require such intense interventions.

Long Description for Figure 12.2
The figure shows two visual communication tools. The first is a picture board with 36 squares, each containing a simple image and a word representing common actions, ideas, or concepts such as like, want, get, make, good, more, not, go, look, turn, help, different, I, he, open, do, put, same, you, she, that, up, all, some, it, here, in, on, can, finished, where, what, why, who, when, and stop. The second tool is a picture exchange communication system; a gray board with removable cards depicting items or activities like squish ball, play doh, screen time, stop, juice, fruit, yogurt, inside, potty, I want, go, and outside. A Velcro strip at the bottom to form phrases and express requests.
Assistive technology services refers to the provision of and commitment to use a variety of devices that help individuals learn and maintain skills, complete activities of daily living, and participate in the community. Examples of assistive technology include screen magnifiers, pencil grips, walkers, and speech-to-text devices. A large subcategory of assistive technology is augmentative and alternative communication (AAC). These types of devices include (but are not limited to) tactile items, such as core boards and the picture exchange communication system (PECS), and digital platforms, like ProLoQuo2Go or Dynavox/TD Snap. A child might use PECS to arrange preferred activities on their visual schedule. Picture boards and PECS can also be loaded into binders or folders in a way that allows various combinations to be accessed for different parts of the day, week, or season. Digital platforms like ProLoQuo2Go go beyond core boards and PECS because they include complementary audio that is more useful as individuals grow and interact with the community beyond the classroom staff.
The clear benefit to communication devices is that they allow an individual with limited or emerging communication skills to express their needs and desires. AACs, particularly digital or tablet-based assistive technology, however, also have drawbacks. Although these platforms are useful in their mobility and ease of use, they require a level of dependence on a device that needs to be charged, is cost prohibitive to repair or replace, has the potential to be used incorrectly, and may have a negative impact on motor development.
12.3 Role of the General Education Teacher
As a general education teacher, particularly in preschool or early elementary settings, the process of accessing the supports that come with special education can be a point of frustration. Early intervention is crucial for social and emotional development. However, federal language (IDEA) mandates us to focus our efforts with students in the LRE and to use caution to avoid overidentification of special education eligibility. Working in collaboration with others can sometimes cause further dissonance as team members may view and prioritize access to resources and adherence to LRE differently. As a classroom teacher, you may need to balance these perspectives by speaking to the strengths and needs of the child. Remember that colleagues in other roles, particularly in special education, may have a different experience or outlook that guides their focus, but they too are child advocates.
Whether or not a child meets criteria for special education eligibility, ongoing documentation is just as important as our collaborative efforts. This means thorough transition planning for children at every grade-level change rather than solely focusing our transition efforts at the program change level. It is just as important for a first-grade teacher to receive thorough documentation from a kindergarten teacher as it is for a kindergarten teacher to receive documentation from a preschool program. Most categories of special education eligibility include criterion language that speaks to ongoing patterns of behavior or vaguely specified lengths of time. Your school, district, or state may have a policy that clarifies its interpretation of IDEA language regarding time frames. Although a child may not be eligible for special education in first grade, your records may help qualify that child for a special education evaluation in second grade after a pattern of behavior or increase in frequency has been documented, along with a list of interventions attempted, and to what degree they were successful.
There is sometimes crossover among supports that are used for a child with an IEP, an IFSP, or a 504 plan. Any support can be made more intensive and individualized for a child who is manifesting a need, whether or not that need has been formalized by federal or local policy. Regardless of where the child is in the eligibility process, the general education teacher can take actionable steps to make all children welcome in their classroom communities, even children with significant behavioral needs. As classroom teachers, part of our role is to create an inclusive classroom community and to collaborate with stakeholders to ensure that all children get the supports they need to engage productively.
Ways that early educators can support all children in our classroom communities through social and emotional development, self-regulation, and behavioral guidance have been woven throughout this text. The community model for classroom management suggests that shifting from a compliance model to one of supportive coregulation positions educators into shared power structures. This shift allows children to be part of solving problems and helps center children in our strategies for confronting difficult situations. Even with these supportive structures, however, finding the bandwidth to successfully navigate behavioral challenges can be emotionally overwhelming. This is especially true when working through classroom or student-specific scenarios with special education students who need intensive supports. Often, there are no quick fixes or simple answers when working with children who exhibit challenging behaviors. If the emotional toll it takes providing intensive services on our own leads to burnout or career change, then the field of education loses a caring and committed educator. It is important to recognize that implementation of intensive supports requires a team approach, and knowing how to ask for assistance can be the most important tool in your behavioral support toolkit.
Key Points
- Children might receive services using IFSPs, IEPs, and 504 plans.
- Some disability categories overlap with a need for intensive supports related to social and emotional development and behavior.
- A number of people, programs, and services are associated with acquiring supports for children who qualify for special education.
- Collaborating with a team of knowledgeable experts to provide supports for students receiving special education services is critical for you as an educator.
Figures
Figure 12.1: Equality vs. equity. Image found via The Inclusion Solution, reused from The Second Line Education Blog by Lamont Douglas, but image’s original creator could not be identified.
Figure 12.2: Picture boards and picture exchange communication systems. (A) Picture board and core board. (B) Picture Exchange Communication System (PECS). (A) The 3D Universal Core Vocabulary Symbols by The Center for Literacy and Disability Studies are licensed CC BY 4.0. Original Picture Communication Symbols copyright 1981–2015 by Mayer-Johnson LLC. (B) Created by Christine Pegorraro Schull with Canva.
Table
Table 12.1: Individualized Education Plan Requirements. Contents adapted from 1.8: The Individualized Education Program in The Psychology of Exceptional Children by Diana Zaleski, licensed CC BY 4.0.
References
Beltrán S., Sit L., & Ginsburg K. R. (2021). A call to revise the diagnosis of oppositional defiant disorder—Diagnoses are for helping, not harming. JAMA Psychiatry, 78(11), 1181–1182. https://doi.org/10.1001/jamapsychiatry.2021.2127
Cloth, A. H., Evans, S. W., Becker, S. P., & Paternite, C. E. (2014). Social maladjustment and special education: State regulations and continued controversy. Journal of Emotional and Behavioral Disorders, 22(4), 214–224. https://doi.org/f6pjzv
Conti, E., Retico, A., Palumbo, L., Spera, G., Bosco, P., Biagi, L., Fiori, S., Tosetti, M., Cipriani, P., Cioni, G., Muratori, F., Chilosi, A., & Calderoni, S. (2020). Autism spectrum disorder and childhood apraxia of speech: Early language-related hallmarks across structural MRI Study. Journal of Personalized Medicine, 10(4), 275. https://doi.org/10.3390/jpm10040275
Francisco, M. P.B., Hartman, M., & Wang, Y. (2020). Inclusion and special education. Education Sciences, 10(9), 238. https://doi.org/10.3390/educsci10090238
Grindal, T., Schifter, L. A., Schwartz, G., & Hehir, T. (2019). Racial differences in special education identification and placement: Evidence across three states. Harvard Educational Review, 89(4), 525–553. https://doi.org/10.17763/1943-5045-89.4.525
Individuals with Disabilities Education Act, 20 U.S.C. § 114 (2004a).
Individuals with Disabilities Education Act, 34 C.F.R. 300.8 (c)(4)(i) (2004b).
Individuals with Disabilities Education Act, 34 C.F.R. §300.320 (b)(a) (2004c).
Individuals with Disabilities Education Act, 34 C.F.R. §303.340 (c)(d) (2004d).
Kincaid, A. P., & Sullivan, A. L. (2017). Parsing the relations of race and socioeconomic status in special education disproportionality. Remedial and Special Education, 38(3), 159–170. https://doi.org/10.1177/0741932516671199
Kubo, K. Y., Iinuma, M., & Chen, H. (2015). Mastication as a stress-coping behavior. BioMed Research International, 876409. https://doi.org/10.1155/2015/876409
Mattson, S. N., Bernes, G. A., & Doyle, L. R. (2019). Fetal alcohol spectrum disorders: A review of the neurobehavioral deficits associated with prenatal alcohol exposure. Alcoholism, Clinical and Experimental Research, 43(6), 1046–1062. https://doi.org/10.1111/acer.14040
Mody, M., & Belliveau, J. W. (2013). Speech and language impairments in autism: Insights from behavior and neuroimaging. North American Journal of Medicine and Science, 5(3), 157–161. https://doi.org/10.7156/v5i3p157
Nanda, J. (2019). The construction and criminalization of disability in school incarceration. Columbia Journal of Race and Law, 9(2), 265–322. https://doi.org/10.7916/cjrl.v9i2.3411
Rehabilitation Act of 1973, Pub. L. No. 93–112, 87 Stat. 355 (1973).
Sallese, M. R., Garwood, J. D., Vannest, K. J., Kolbe, T., & Carlson, A. (2024). Definitions of and evaluation procedures for emotional disturbance: A tale of 50 states. Behavioral Disorders, 49(2), 106–115. https://doi.org/10.1177/01987429231215352
Section 504 of the Rehabilitation Act of 1973, 34 C.F.R. Part 104.
Smiley, L. R., Richards, S. B., & Taylor, R. (2022). Exceptional students: Preparing teachers for the 21st century (4th ed.). McGraw Hill.
U.S. Department of Education, Office for Civil Rights. (2010). Free appropriate public education for students with disabilities: Requirements under Section 504 of the Rehabilitation Act of 1973.
