
An Introduction to Community and Public Health Nursing
Overview
The focus of this chapter is to provide an overview of community and public health nursing and highlight its importance in protecting, preserving, and promoting the public’s health and safety. The different levels of disease prevention are presented and discussed in consideration of the social determinants of health and health promotion. The chapter provides the common ethical frameworks and theories that guide the work of public and community health nurses.
Learning Objectives
- Define community and public health nursing
- Discuss the roles and settings of public health nurses
- Differentiate between primordial, primary, secondary, tertiary, and quaternary prevention
- Identify the major nursing, social, and public health theories that guide community health education, promotion, and prevention programs
- Identify community health nursing roles and practice settings
- Discuss the ethical principles that guide and influence community health nursing
Key Terms
- public health nursing
- community health nursing
- vulnerable populations
- primordial prevention
- primary prevention
- secondary prevention
- tertiary prevention
- quaternary prevention
Introduction
The success or failure of any government, in the final analysis, must be measured by the well-being of its citizens. Nothing can be more important to a state than its public health; the state’s paramount concern should be the health of its people.
—Franklin Delano Roosevelt (Quoted in Gostin, 2000).
Public and community health nursing is a unique aspect of nursing practice. Nurses who work in the community must develop a broad array of knowledge and skills that inform a collaborative approach to improving the health of individuals, families, and whole communities. Community health nurses work directly with community members in roles like home health and school nursing or through community-based organizations. Public health nurses tend to work with city or state institutions such as the public health department. Though many provide direct care through clinics, many also work to achieve local or statewide population-level health goals. In this chapter, you will learn more about the roles of community and public health nurses, the populations of people they work with, and the overarching approaches to this type of work.
Public and Community Health Nursing
The American Public Health Association defines public health nursing as “the practice of promoting and protecting the health of populations using knowledge from nursing, social and public health sciences” (American Nurses Association [ANA], 2022). Community health nursing is a subset of public health nursing but focuses on specific communities, usually defined in geographic terms. The term community health nurse is often used to define a role (e.g., school nurse) more specifically. The public health nurse encompasses the roles of community health nurses but also includes roles that focus on broader interventions that affect whole populations. Throughout this book, the terms public health nurse and community health nurse are both used. As individuals, nurses directly influence the health and well-being of patients every day. Through frequent contact, nurses are best placed to encourage lifestyle changes in communities and offer education on healthy living, particularly to the most vulnerable in society.
Nurses often work with community partners to address the health of vulnerable populations—those whose health is adversely affected because of their varying access to health care or lack of access to equal social opportunities. This inability to access health care could result from their socioeconomic status, culture, ethnicity, or health status (Waisel, 2013). Some examples of vulnerable populations in the United States are these:
- Racial or ethnic minority members
- Immigrants/refugees/asylees
- Children
- Older adults
- Socioeconomically disadvantaged individuals
- People experiencing homelessness
- Underinsured or uninsured individuals
- Persons who are incarcerated
- Veterans
- LGBTQIA+ population
- Those in certain geographical communities (e.g., Indian reservations, rural)
- Persons who are chronically ill or disabled (Joszt, 2018; Waisel, 2013)
By working collaboratively with community members and key stakeholders, nurses can greatly affect public health as a whole. Nurses can facilitate communication and establish cooperative processes to create inclusive environments. Each community has unique characteristics. Effective community nursing embraces community uniqueness and assists community members to take active leadership roles in determining and addressing needs. During collaborations, community characteristics such as language and cultural preferences may become barriers to effective problem-solving. Nurses can take a lead role as facilitator and advocate to ensure that high-quality communication between all parties is clear and that the community members’ perspectives are centered. Nurses who follow the key principles of community health nursing do the following:
- Emphasize primary prevention
- Work to achieve the greatest good for the largest number of individuals
- Recognize that the client is a partner in health
- Practice cultural humility
- Use resources wisely to promote the best outcomes
Public Health Nursing Roles and Settings
Major Roles
In any setting, the role of public health nurses focuses on the prevention of illness, injury, or disability; the promotion of health; and the maintenance of the health of populations. The community health nurse’s role is to integrate public health knowledge into their nursing practice by applying the nursing process of assessment, diagnosis, planning, implementation, and evaluation, commonly referred to as ADPIE (Toney-Butler & Thayer, 2022). Doing this requires incorporating knowledge regarding the social determinants of health (SDOH) in caring for individuals, families, communities, and populations. These determinants of health can be defined as socioeconomic factors with significant direct or indirect impacts on health (Braveman et al., 2011).
Examples of public health nursing activities include the following:
- Evaluating health trends and risk factors of population groups and helping to determine priorities for targeted interventions
- Collaborating with communities or specific population groups within the community to develop public policy and targeted health promotion and disease prevention activities
- Participating in assessing and evaluating health care services to ensure that people are informed of available programs and services and assisted in the utilization of those services
- Providing essential input to interdisciplinary programs that monitor, anticipate, and respond to public health problems in population groups
- Providing health education, care management, and primary care to individuals and families who are members of vulnerable populations and high-risk groups (Missouri Department of Health & Senior Services, 2022)
Community health nurses practice in various settings, including community clinics, government agencies, outpatient clinics, school systems, and nonprofit organizations.
Health Department Services
The Structure of Health Departments
The U.S. Department of Health and Human Services is a federal agency whose aim is to protect all American people. It is the parent agency for many other agencies, including the Centers for Disease Control and Prevention (CDC). The purpose and function of the CDC reflect the purpose of local health departments.
Public health departments, states, and localities use different governing systems at the local level. There are four main structures for governance:
- Centralized: State employees lead the health units.
- Decentralized: Local (city or county) employees lead the health units.
- Mixed structure: Some local health units are led by employees of the state and some are led by employees of local government. No single structure predominates.
- Shared: Local health units might be led by either state or local employees. If health departments are led by state employees, then the local government has the authority to make financial decisions and/or issue public health orders; if they are led by local employees, then the state has authority (CDC, 2021a).
The Purpose and Function of Health Departments
The key principles of public health nursing work within the framework offered by the CDC’s 10 Essential Public Health Services, which protect and promote the health of all people in all communities. To achieve equity, the 10 Essential Public Health Services actively promote policies, systems, and overall community conditions that enable optimal health for all and seek to remove systemic and structural barriers resulting in health inequities. Such barriers include poverty, racism, gender discrimination, ableism, and other forms of oppression. The 10 Essential Public Health Services stipulate that public health care providers do the following:
- Assess and monitor population health status, factors that influence health, and community needs and assets
- Investigate, diagnose, and address health problems and hazards affecting the population
- Communicate effectively to inform and educate people about health, factors that influence it, and how to improve it
- Strengthen, support, and mobilize communities and partnerships to improve health
- Create, champion, and implement policies, plans, and laws that affect health
- Utilize legal and regulatory actions designed to improve and protect the public’s health
- Assure an effective system that enables equitable access to the individual services and care needed to be healthy
- Build and support a diverse and skilled public health workforce
- Improve and innovate public health functions through ongoing evaluation, research, and continuous quality improvement
- Build and maintain a strong organizational infrastructure for public health (CDC, 2021b)
The core functions of public health—assessment, policy development, and assurance—provide the structure for assessing public health performance and serve as the basis for these 10 Essential Public Health Services. These services, shown in Figure 2, offer the framework for carrying out the mission of public health nursing and describe the activities that all communities should undertake (CDC, 2021b).
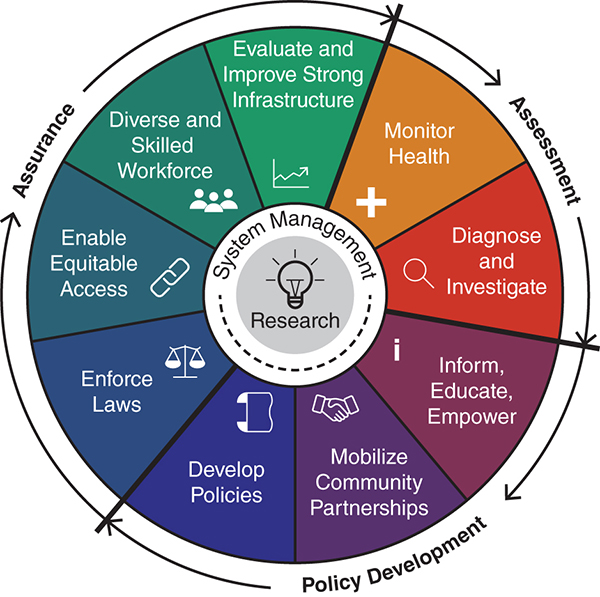
Long Description for Figure 2
Assessment: Monitor health. Diagnose and investigate. Development: Inform, educate, and empower. Mobilize community partnerships. Develop policies. Assurance: Enforce laws. Enable equitable access. Diverse skilled workforce. Evaluate and improve strong infrastructure. The center of the framework shows system management centered around research.
Local public health agencies provide services at the community and individual levels. Local health departments have a fundamental and complex role as the front line for the delivery of basic public health services to most of the communities in this country. Health departments provide services that include emergency preparedness and response, immunizations, environmental health, infectious disease prevention, food safety, maternal and child health, tobacco control, and injury and violence prevention (National Association of County and City Health Officials, 2017). Through primary, secondary, and tertiary prevention strategies, local health departments promote and protect the health of the people and the communities where they live and work (Figure 3).
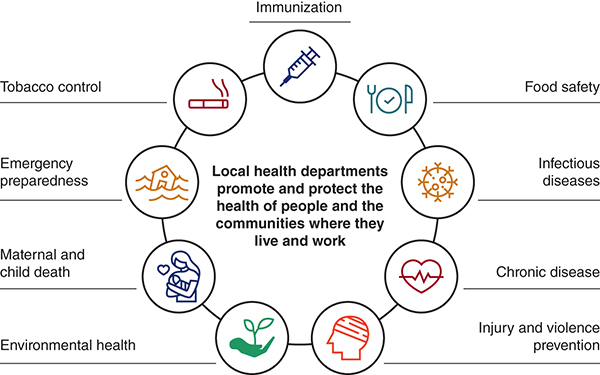
Long Description for Figure 3
The services include the following. Immunization. Food safety. Infectious diseases. Chronic diseases. Injury and violence prevention. Environmental health. Maternal and child health. Emergency preparedness. Tobacco control.
Disease Prevention
Primordial, Primary, Secondary, Tertiary, and Quaternary Prevention
Prevention focuses on improving the public’s health through avoiding disease, reducing disease severity, and promoting health rather than only treating disease. Prevention strategies address the five distinct stages of illness:
- Underlying
- Susceptible
- Subclinical
- Clinical
- Recovery/disability/death (Kisling & M Das, 2022)
Prevention strategies for each stage of illness are divided into four levels: primordial, primary, secondary, and tertiary (Figure 4). These strategies are intended to prevent disease and reduce associated risk and complications from its progression. The health of the American public has improved in some ways over the last decades, but many diseases and illnesses are still increasing in frequency (CDC, 2019). Reasons for these increases are often unknown, making prevention an important element of disease management.
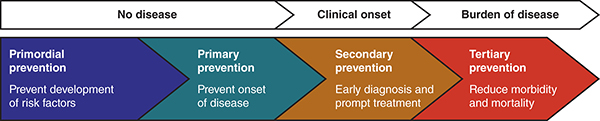
Long Description for Figure 4
No disease: primordial prevention to prevent the development of risk factors; primary prevention to prevent onset of disease. Clinical onset: Secondary prevention that focuses on early diagnosis and prompt treatment. Burden of disease: Tertiary prevention that focuses on reducing morbidity and mortality.
Primordial Prevention
The newest level of prevention, primordial prevention, involves identifying social and environmental variables that can influence the health of entire populations and implementing targeted risk reduction strategies (Kisling & M Das, 2023). These efforts are often advanced by laws and public policy. Primordial prevention is designed to address underlying stages of the disease by considering SDOH. The purpose of primordial prevention is to modify SDOH by addressing factors that are understood to increase the risk of future diseases, such as environmental, economic, social, and behavioral conditions. These strategies seek to inhibit risk factors at a systemic level rather than at the individual, personal level (CDC, 2019).
Examples of primordial prevention include these:
- Government policy—increasing taxes on cigarettes, decreasing advertisement of tobacco
- Built environment—increasing access to safe walking paths, increasing access to stores with healthy food options
- Health promotion—increasing the affordability of programs and activities that maximize health, increasing activity, and promoting weight reduction (CADI Research Foundation, 2012; Kisling & M Das, 2023)
Primordial prevention policies are population-based strategies for prevention. Strategies aimed at lowering risk factors of the entire population are focused on modification of lifestyle with three major lifestyle changes being primarily targeted: smoking cessation, healthy diet, and increased physical activity. Substantial health improvement can result from relatively small costs in these areas. Promoting a healthy lifestyle in the population can be encouraged by helping people seek alternatives and making those alternatives available. Implementing many primordial, evidence-based interventions requires an established long-term policy framework and appropriate institutional support. The goal of primordial prevention is to create future generations who experience fewer health risks and enjoy a greater state of wellness. Public health nurses can participate in primordial prevention by becoming change agents through participating in policy creation and review to protect population health (Villa et al., 2021).
Primary Prevention
Primary prevention strategies are designed to intervene before illness occurs (CDC, 2019). They may include actions to improve health, such as providing information on behavioral and medical health risks, giving guidance, and suggesting measures to decrease health risks at the personal and community level. Primary prevention focuses on measures targeting a susceptible population or individual. The purpose of primary prevention is disease prevention through actions and strategies designed to prevent disease from beginning in the first place. As such, the target population is healthy individuals and communities. Primary prevention is aimed at limiting risk exposure. In addition, primary prevention prioritizes programs and interventions designed to increase the immunity of at-risk individuals in order to prevent a disease from progressing to subclinical disease (Kisling & M Das, 2023).
Primary prevention includes actions targeted at avoiding the manifestation of a disease. This may include any of the following ways to improve health:
- A change in the degree of influence and impact of social and economic determinants on health
- Provision of information and intervention programs on behavioral and medical health risks, in addition to consultation and measures to reduce risk at the personal and community level
- Nutritional and food supplementation programs
- Oral and dental hygiene education
- Clinical preventive services such as immunization and vaccination of children, adults, and the elderly, as well as vaccination or postexposure prophylaxis for people exposed to a communicable disease (World Health Organization [WHO], n.d.)
Public health nurses participate in primary prevention when they participate in vaccination outreach clinics, nutrition education, food access programs, or any other activity designed to prevent the onset of disease at the individual, family, or community level. Nurses also play an essential role in educating people about the adoption of healthy lifestyle choices such as embracing good nutrition, avoiding smoking, engaging in physical activity, and investing in strategies for stress reduction (Vellone, 2016).
Secondary Prevention
Secondary prevention targets early disease detection to improve the chances of positive health outcomes. Secondary prevention aims to detect a disease or condition in an asymptomatic stage and prevent progression to symptomatic disease. Early diagnosis and prompt treatment assist in preserving health. Many diseases found early may be cured without residual complications and pathologies. Often individuals can return to full health (AbdulRaheem, 2023). Secondary prevention also aims to prevent the spread of disease to other individuals and limit the expected disability to prevent potential future inactivity and dependence. While primary prevention activities may be implemented independently of other advances and support structures in other health care services, this is not so for secondary prevention. The benefits of screening and early detection are limited without access to other parts of the health care system. Nurses are the primary caregivers in many diverse and different health care settings and play a significant role in conducting secondary prevention, often serving as a liaison between participants and other professionals. Nurses’ perceptions of the barriers to and enablers of secondary prevention help create better understanding of the influencing factors of secondary prevention while contributing to enhanced secondary prevention program design (Ni et al., 2022).
Public health nurses participate in secondary disease prevention services and such activities as:
- Evidence-based screening programs for early detection of congenital malformations
- Blood pressure screening
- Community screening of HGA1C, which can identify prediabetic states
- Hearing screenings for children under age 5 (WHO, 2022)
Tertiary Prevention
Tertiary prevention focuses on both the clinical and outcome stages of a disease. It aims to reduce the severity of disease in symptomatic patients and make living easier with long-term health problems and injuries. Tertiary prevention aims to modify the negative consequences of an already established disease and focuses on measure to restore function through mental, physical, and social restoration and rehabilitation. Tertiary prevention intends to improve the quality of life by reducing disability, limiting or delaying complications, and restoring function. The following are some examples of tertiary prevention:
- Disease management activities: Disease management activities of chronic conditions such as hypertension, diabetes, asthma, or heart disease are best examples. Strategies focus on lifestyle changes, medication management, and routine physicals. They are implemented by the provision of education, self-care practices, and regular monitoring and are intended to assist persons in controlling their condition, fostering patient compliance, maturing self-efficacy, and avoiding future consequences.
- Rehabilitation activities: Rehabilitation interventions play a crucial role in supporting individuals who have experienced a significant injury and are designed to help these individuals regain lost functions and skills. These interventions often include physical therapy to restore mobility, occupational therapy to regain independence in daily activities, and speech therapy to enhance communication abilities.
- Pain management: Pain management strategies are unique tertiary prevention measures designed to help individuals coping with chronic pain conditions. The primary goal of comprehensive pain management is the reduction and/or alleviation of pain in contribution to an overall better quality of life. (AbdulRaheem, 2023)
Nurses participate in many tertiary prevention programs. Among their responsibilities are these:
- Managing outpatient and home-based cardiac or stroke rehabilitation programs
- Leading evidence-based community chronic disease management programs
- Leading support groups that allow members to share strategies for living well
Quaternary Disease Prevention
Quaternary disease prevention includes action taken to identify patients at risk for overtreatment. It is a more recent concept designed to identify persons at risk of excessive medicalization who therefore afford protection from further unnecessary interventions, including avoiding iatrogenic damages. These individuals may be open to suggestions about ethically acceptable alternative measures. Quaternary prevention requires physicians, health professionals, and managers of health systems to critically evaluate themselves and their activity. To be successful, this reflection should include an operational consideration that includes the questioning of technical and ethical limits. The intent is to heighten self-awareness regarding influences that affect decisions. Quaternary prevention is focused on prospective constructs of good practices without cultural, technical, and institutional bias, which can prove harmful to the health of an individual or the health of the population as a whole. The objective of this type of prevention is to influence the action of professionals and health systems (Tesser, 2017). Nurses have the unique opportunity as a function of their patient advocacy role to encourage patients to actively participate in their health care decisions. Nurses practice good advocacy through first establishing an effective and transparent communication and trust relationship with patients and by then becoming and remaining aware of patients’ legal rights, with the aim of protecting these rights.
Public health nurses support quaternary prevention strategies by doing the following:
- Completing medication review and reconciliation to prevent unnecessary polypharmacy
- Initiating conversations and assisting in completing advance medical directives
- Empowering individuals, families, and communities to be active and equal participants in their care, seeking second opinions when necessary
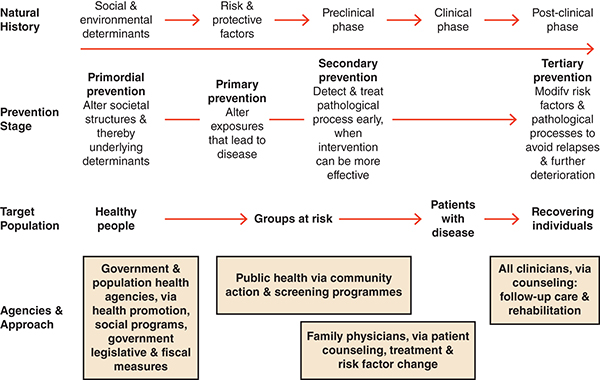
Long Description for Figure 5
The Natural History begins with social and environmental determinants that contribute to risk and protective factors, moving through the preclinical and clinical phases, and eventually reaching the post-clinical phase. The Prevention Stage is divided into four key phases. Primordial prevention focuses on altering societal structures and underlying determinants to reduce risk factors. Primary prevention aims to alter exposures that could lead to disease. Secondary prevention involves early detection and treatment of pathological processes when outcomes can be more effective. Finally, tertiary prevention seeks to modify risk factors and pathological processes to avoid relapses and further deterioration. The target population starts with healthy individuals and transitions to groups at risk, then to patients with disease, and ultimately to recovering individuals. The agencies and approach employ the various organizations and methods that support disease prevention and treatment. Government and population health agencies play a crucial role in health promotion, social programs, and legislative measures. Public health organizations are involved in community action and screening programs. Family physicians focus on patient counseling, treatment, and addressing risk factors. Finally, all clinicians are involved in follow-up care, counseling, and rehabilitation to support recovering individuals.
Health Promotion
In addition to engaging in prevention strategies to increase the health of communities, public health nurses also engage in health promotion. A working definition for health promotion was presented during the First International Conference of Health Promotion conducted in Ottawa, Canada. Health promotion was defined as “the process of enabling people to increase control over, and to improve, their health” (WHO, 1986). Health promotion involves encouraging, guiding, and supporting people in choosing healthy lifestyle behaviors through health literacy. Health promotion applies to individuals, the community-at-large, or vulnerable populations. Examples of public health nursing engaging in health promotion are:
- Building health literacy
- Participating in health campaigns, like knowing the signs of a stroke or performing regular self-exams
Impacts of Prevention Strategies
Prevention strategies and health promotion have an impact beyond the individual. The CDC outlines essential benefits of prevention strategies to communities, including:
- Health status and health disparities. Any intervention that directly or indirectly affects the determinants of health will also affect the community’s health, reducing the likelihood of disparity between populations.
- Health care costs. Prevention strategies can also have an impact on health care costs. When a positive change affects an entire community, that community’s overall medical care costs go down.
- Non-health impact. Many health prevention interventions have impacts on other sectors of people’s lives. Non-health impacts can improve people’s ability to increase their “well” days where they can work or enjoy recreational activities that increase their income or sense of well-being. (Miller et al., 2015)
Ethics
Ethical practice is essential because nurses deal with ethical issues daily. Ethical dilemmas arise as nurses care for patients. These dilemmas may sometimes conflict with the ANA Code of Ethics or the nurse’s ethical values. Nurses are advocates for patients and must find a balance while delivering patient care (Haddad & Geiger, 2022).
Ethical considerations in nursing, though challenging, represent a true integration of the art of patient care. Nurses are responsible for themselves, their profession, and their patients to maintain the highest ethical principles. Some organizations have ethics boards in place to review ethical concerns. Public health nurses have an ethical imperative to advocate for patient care, patient rights, and ethical consideration of practice. Ethics inclusion should begin in nursing school and continue in nursing practice.
Community health nurses are guided by the ANA Code of Ethics and other principles and theories, including social justice theories (Pope et al., 2016; ANA, 2016).
Social Justice
Social justice is based on the application and distribution of equity rights, access, and participation within a society focused on countering oppression and powerlessness. In terms of social justice, the role of public health nurses is to support the inclusion of people living on the margins of society, helping empower them to freely participate on an equal footing of respect (Vollman, 2004). Social justice in health care translates to the delivery of high-quality care to all individuals. Achieving social justice is critical to equitable health and health care that ensures all individuals can maintain their highest level of health and wellness (Pope et al., 2016).
Theory and Frameworks
The ANA Code of Ethics for Nurses
The ANA has developed a comprehensive code of ethics that clarifies the profession’s primary goals, values, and obligations. The ANA code is an ethical decision-making framework. For all nurses, this code stands as a succinct statement of the ethical obligations and duties of every individual who enters the nursing profession. Nurses should know and demonstrate these principles within their practice (ANA, 2015).
Ethical values are universal rules of conduct that serve as a basis for discerning which actions, intentions, and motives are valued. Ethics are the guiding “moral principles that govern how the person or group will behave or conduct themselves” (Haddad & Geiger, 2022). The focus of ethics is to provide a guide for the right and wrong actions and their consequences when engaging in the decision-making process. Although individuals possess their own set of ethics, morals, and values, many professional organizations have developed a set of ethical principles to guide competent practice with integrity and good judgment. “Ethics within healthcare are important because workers must recognize healthcare dilemmas, make good judgments and decisions based on their values while keeping within the laws that govern them” (Haddad & Geiger, 2022).
There are currently nine provisions for the ANA Code of Ethics that guide nursing practice. The following is a summary:
- Provision 1. The nurse practices with compassion and respect for every person’s inherent dignity, worth, and unique attributes.
The nurse must provide care to all individuals with demonstrated dignity and respect while valuing their unique attributes. This means that care must be personalized to meet the needs of the individual.
- Provision 2. The nurse’s primary commitment is to the patient, whether an individual, family, group, community, or population.
The nurse should consider the patient as a primary concern while addressing their concerns and encouraging their active participation in their care. Conflicts of interest, at whatever level, should not influence patient care. The nurse must be open to collaborating while maintaining professional boundaries to maximize the level of care provided to the patient.
- Provision 3. The nurse promotes, advocates for, and protects patients’ rights, health, and safety.
The nurse must comprehend and guard all privacy and confidentiality guidelines to protect the patient. The nurse must ensure that informed consent is obtained when needed. The nurse involved in research must ensure that they are well versed in the protection of human subjects and that all safeguards include full disclosure for patients agreeing to participate in research studies and the maintenance of patient privacy and anonymity. The nurse must adhere to all established standards of practice and maintain a high level of competence using current evidence-based interventions.
- Provision 4. The nurse has authority, accountability, and responsibility for nursing practice; makes decisions; and acts consistent with the obligation to provide optimal patient care.
The nurse must utilize their authority in an ethical, professional manner. The nurse must responsibly engage in well-thought-out, planned, and purposeful decisions. Delegation of nursing activities or functions must be done with respect for the patient and the actions required to ensure appropriate delegation to one who is qualified and capable of completing the task.
- Provision 5. The nurse owes the same duties to themself as to others, including the responsibility to promote health and safety, preserve wholeness of character and integrity, maintain competence, and continue personal and professional growth.
The nurse must demonstrate care for self as well as others. The nurse should be concerned for personal and professional growth and development.
- Provision 6. Through individual and collective effort, the nurse establishes, maintains, and improves the ethical environment of the work setting and conditions of employment that are conducive to safe, quality health care.
The nurse is responsible for establishing, maintaining, and improving the ethical, safe, quality work that offers high-quality care.
- Provision 7. In all roles and settings, the nurse advances the profession through research and scholarly inquiry, professional standards development, and nursing and health policy generation.
The nurse must be willing to engage with scholarly inquiry and research and advocacy for and generation of nursing and health policy. The nurse’s educational experience should include research principles, and each nurse should understand how to apply scholarly work and inquiry into practice standards.
- Provision 8. The nurse collaborates with other health professionals and the public to protect human rights, promote health diplomacy, and reduce health disparities.
The nurse must collaborate with colleagues in nursing and other disciplines to maximize patient outcomes, promote health diplomacy, protect human rights, and reduce health disparities within their sphere of influence.
- Provision 9. The profession of nursing, collectively through its professional organization, must articulate nursing values, maintain the profession’s integrity, and integrate principles of social justice into nursing and health policy.
The nurse is responsible for participating in professional organizations with a willingness to become a voice for social justice and the advancement of the nursing profession. The nurse must maintain political awareness to maintain the integrity of the nursing profession. The nurse should willingly contribute to health policy advocacy, which should be shared among the profession, joining nurses worldwide for a unified voice (Haddad & Geiger, 2022).
Sufficiency of Well-Being
Powers and Faden’s (2008) theory of sufficiency of well-being presents social justice as the moral foundation of public health. Their model identifies a six-dimensional theory of well-being that considers ethical issues in public health and health policy development. There are six core dimensions:
- Health
- Personal security
- Reasoning
- Respect
- Attachment
- Self-determination
Ethical Theory of Population-Focused Nursing
Derryl Block and Lavohn Josten, public health educators, proposed the ethical theory of population-focused nursing based on intersecting public health and nursing fields. In their framework, there are three essential elements relevant to public health nursing:
- An obligation to the population
- The primacy of prevention
- The centrality of relationship-based care (Current Nursing, 2020)
Social-Ecological Model
The social-ecological model considers the complex interrelationships between individuals, relationships, community, and societal factors. The overlapping rings in the model illustrate how factors at one level influence factors at another level (Figure 6). The model suggests a bidirectional relationship between individuals, families, communities, and society (CDC, 2022). Nursing interventions using the social-ecological model must consider all four levels.
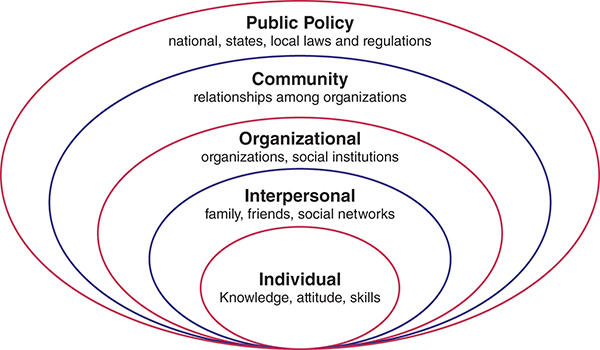
Long Description for Figure 6
Individual: knowledge, attitude, and skills. Interpersonal: family, friends, and social networks. Organizational: organizations, and social institutions. Community: the relationships among organizations. Public policy: national, state, and local laws and regulations.
Individual: The first level identifies biological and personal history factors that increase the likelihood of becoming a victim or perpetrator of violence. Among these factors are age, education, income, substance use, or history of abuse. Prevention strategies at this level promote attitudes, beliefs, and behaviors that prevent violence. Specific approaches may include conflict resolution and life skills training, social-emotional learning, and safe dating and healthy relationship skill programs.
Relationship: The second level examines close relationships that may increase the risk of experiencing violence as a victim or perpetrator. A person’s closest social circle—peers, partners, and family members—influences their behavior and contributes to their experience. Prevention strategies at this level may include parenting or family-focused prevention programs and mentoring and peer programs designed to strengthen parent–child communication and promote positive peer norms, problem-solving skills, and healthy relationships.
Community: The third level explores the settings, such as schools, workplaces, and neighborhoods, in which social relationships occur and seeks to identify the characteristics of these settings that are associated with becoming victims or perpetrators of violence. Prevention strategies at this level focus on improving the physical and social environment in these settings (e.g., by creating safe places where people live, learn, work, and play) and addressing other conditions that give rise to violence in communities (e.g., neighborhood poverty, residential segregation and instability, high density of alcohol sales and service outlets).
Societal: The fourth level looks at the broad societal factors that help create a climate in which violence is encouraged or inhibited. These factors include social and cultural norms that support violence as an acceptable way to resolve conflicts. Other large societal factors include the health, economic, educational, and social policies that help to maintain economic or social inequalities between groups in society. Prevention strategies at this level include efforts to promote societal norms that protect against violence as well as efforts to strengthen household financial security, provide education and employment opportunities, and foster other policies that affect SDOH (CDC, 2022).
Health Belief Model
The health belief model (Figure 7) states that health-related behavior depends on perceptions in four areas:
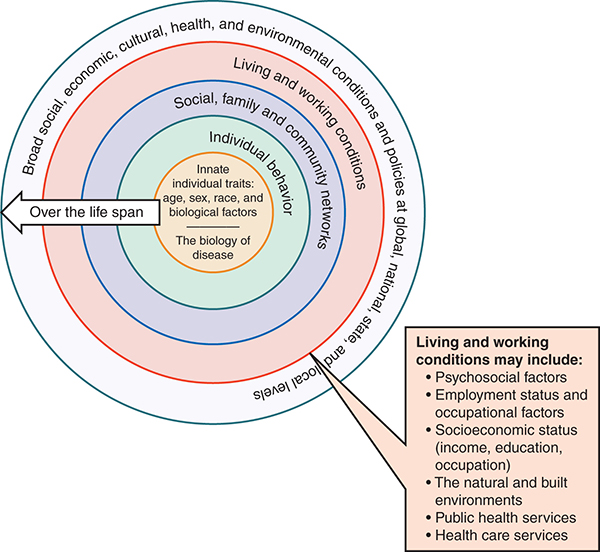
Long Description for Figure 7
The innermost circle represents the biology of disease, innate individual traits such as age, sex, race, and biological factors affect health. The next circle represents individual behavior. The next circle represents the social, family, and community networks, followed by living and working conditions, which may include psychosocial factors, employment status, occupational factors, socioeconomic status including income, education, occupation, natural and built environments, public health services, and healthcare services. The outermost circle represents broad social, economic, cultural, health, and environmental conditions and policies at global, national, state, and local levels.
- The severity of a potential illness
- An individual’s susceptibility to that illness
- Benefits of taking preventive action
- The barriers to taking that action (Hochbaum, 1958; Rosenstock, 1960, 1966)
The model also uses the idea of using cues to action. For example, someone might set an alarm to remember to take their medication or to take a walk (Becker, 1976). The health belief model also includes the construct of self-efficacy. Self-efficacy means a person’s confidence in their ability to successfully perform healthy behavior (Rosenstock, 1990).
Transtheoretical Model
The transtheoretical model of behavior change is a five-stage cycle about readiness to change (Prochaska et al., 1992):
- Precontemplation
- Contemplation
- Preparation
- Action
- Maintenance (Prochaska & DiClemente, 1982, 1984)
In the transtheoretical model, efficient self-change depends on doing the right thing (processes) at the right time (stages; Prochaska et al., 1992). Nurses can apply this model in the public setting by customizing interventions to match a person’s readiness or stage of change (Marcus & Owen, 1992).
Theory of Reasoned Action
Public health nurses continue to use the theory of reasoned action (Ajzen & Fishbein, 1980; Ajzen & Fishbein, 1975) in health promotion programming. This theory presents the idea that individuals’ behaviors are determined by their intent to perform that behavior.
Further, that intention is determined by two major factors: first, the person’s attitude toward the behavior; and second, the influence of the person’s social environment or subjective norm. This means that public health nurses should assess attitudes toward health behavior changes as well as the attitudes of others that may influence the individual. Public health nurses can use this theory when they are working to change attitudes at the community level or helping individuals identify their own health priorities and willingness to make health behavior changes.
Theory of Planned Behavior
The theory of planned behavior (Ajzen, 1985, 1988) builds on the theory of reasoned action to include the concept of perceived control over the opportunities, resources, and skills that are necessary to perform a behavior. Ajzen’s perceived behavioral control construct is similar to Bandura’s (1977) concept of self-efficacy. Public health nurses can apply this theory to empower clients and communities to identify the elements they feel necessary to succeed in health behavior change.
Healthy People 2030
Healthy People 2030 is overseen by the Office of Disease Prevention and Health Promotion (ODPHP), Office of the Assistant Secretary for Health, and the Office of the Secretary (ODPHP, 2022a). Healthy People is updated each decade and provides data-driven goals and objectives aimed at improving the health of all. Healthy People 2030 operates on a framework developed by the Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2030. The framework aims to provide historical context, locate the current initiatives, and clearly communicate the foundation tenets of the initiatives, principles, context, and rationale for the Healthy People’s approach (ODPHP, 2022b).
The Social Determinants of Health
A focus of the Healthy People framework is now on SDOH. Broadly speaking, social determinants are where we are born and where we grow up, go to school, pray, and play. HealthyPeople.gov arranges SDOH into five categories. These are economic stability, education access and stability, health care access and quality, neighborhood and built environment, and social and community context. By shifting focus to include SDOH, we can understand how “upstream” elements like policies and society-level views can affect the health of populations and individuals. What is important to note here is that because of systemic influences, individual health behaviors do not have equal impact across all populations. Figure 8 provides an example of system (upstream) to individual (downstream) social elements that act as health determinants.
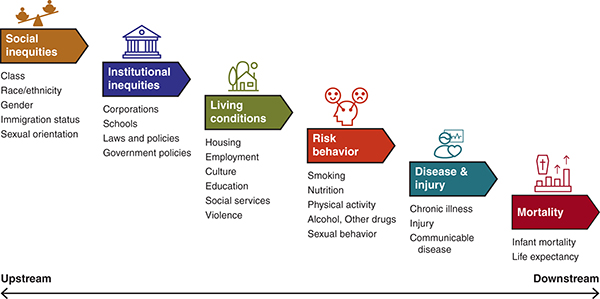
Long Description for Figure 8
The social elements, in the order from the left to right, are as follows. Social Inequities: class, race or ethnicity, gender, immigration status, and sexual orientation. Institutional Inequities: corporations, schools, laws and policies, and government policies. Living Conditions: housing, employment, culture, education, social services, and violence. Risk Behavior: smoking, nutrition, physical activity, alcohol, other drugs, and sexual behavior. Disease and Injury.chronic illness, injury, and communicable diseases. Mortality; It includes infant mortality and life expectancy.
Practice Application
➔ Setting the Scene
As a part of a review of homelessness in the area, the Pleasant City Council has convened a task force to evaluate the need for homeless shelters in the city. Results of the task force’s community assessment showed that while more men than women are currently without housing in the city, the percentage of homeless women is steadily rising. Assessment findings also showed that more women with children live in poverty than men. The task force found that many women who are living in poverty are being overlooked and, as a result, are at risk of becoming unhoused.
Pleasant already has a homeless shelter for men. Based on the information gathered from the community assessment, the task force and the Pleasant City Council have decided to open a homeless shelter designed to primarily serve women with children who are unhoused or in poverty.
➔ Think About It
Imagine you are a community health nurse serving on the task force. You and other task force health care professionals are charged with planning health care services for women with children to be provided at the new homeless shelter.
- What common health problems should you and the task force be aware of when planning which health services to provide at the new shelter?
- What health determinants influence the health of the residents who will be cared for in the new homeless shelter?
- What are some suggestions for primordial, primary, secondary, or tertiary disease prevention strategies to support the residents of the new homeless shelter? How might you help these residents participate in these efforts?
- After the shelter opens, you become one of the nurses who work in the clinic. What strategies are important for you to implement when working with this population?
- Drawing on the Healthy People 2030 recommendations for health policy advancement, where and how should you become an advocate for change?
Additional Resources
American Nursing Association, ANA Code of Ethics
References
AbdulRaheem, Y. (2023, January–December). Unveiling the significance and challenges of integrating prevention levels in healthcare practice. Journal of Primary Care Community Health, 14, 21501319231186500. https://doi.org:10.1177/21501319231186500
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & J. Beckmann (Eds.), Action control: From cognition to behavior (pp. 11–39). Springer Berlin Heidelberg. https://doi.org/10.1007/978-3-642-69746-3_2
Ajzen, I. (1988). Attitudes, personality and behavior. Open University Press./z-wcorg/
Ajzen, I., & Fishbein, M. (1975). A Bayesian analysis of attribution processes. Psychological bulletin, 82 (2), 261.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Prentice Hall; Englewood Cliffs, NJ.
American Nurses Association. (2015). Code of ethics for nurses with interpretive statements./z-wcorg/
American Nurses Association. (2016). The nurse’s role in ethics and human rights: Protecting and promoting individual worth, dignity, and human rights in practice settings. https://www.nursingworld.org/practice-policy/nursing-excellence/official-position-statements/id/the-nurses-role-in-ethics-and-human-rights/
American Nurses Association. (2022). Public health nursing. www.nursingworld.org/practice-policy/workforce/public-health-nursing
Association of Faculties of Medicine of Canada. (2022). Chapter 4: Basic concepts in prevention and health promotion. AFMC primer on population health. https://phprimer.afmc.ca/en/part-i/chapter-4/
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. https://doi.org/10.1037//0033-295x.84.2.191
Becker, M. H. (1976). The health belief model and personal health behavior. C. B. Slack./z-wcorg/
Braveman, P., Egerter, S., & Williams, D. R. (2011). The social determinants of health: Coming of age. Annual Review of Public Health, 32(1), 381–398. https://doi.org/10.1146/annurev-publhealth-031210-101218
CADI Research Foundation. (2012). Primordial prevention. https://cadiresearch.org/topic/prevention-and-control/primordial-prevention
Centers for Disease Control and Prevention. (2019). Picture of America: Prevention. https://web.archive.org/web/20240314114100/http://www.cdc.gov/pictureofamerica/pdfs/Picture_of_America_Prevention.pdf
Centers for Disease Control and Prevention. (2021a). Health department governance. https://web.archive.org/web/20240222235437/https://www.cdc.gov/publichealthgateway/sitesgovernance/index.html
Centers for Disease Control and Prevention. (2021b, March 18). 10 Essential public health services. www.cdc.gov/publichealthgateway/publichealthservices/essentialhealthservices.html
Centers for Disease Control and Prevention. (2022). The social-ecological model: A framework for prevention. https://www.cdc.gov/violence-prevention/about/?CDC_AAref_Val=https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html
Centers for Disease Control. (2024, January 8). 10 Essential public health services. Retrieved January 8, 2024, from https://www.cdc.gov/publichealthgateway/publichealthservices/essentialhealthservices.html
Current Nursing. (2020). Theories applied in community health nursing. https://currentnursing.com/nursing_theory/theories_community_health_nursing.html
Dahlberg, L. L., & Krug, E. G. (2002). Violence: A global public health problem. In E. Krug, L. L. Dahlberg, J. A. Mercy, A. B. Zwi, & R. Lozano (Eds.), World report on violence and health (pp. 1–21). World Health Organization.
Gostin, L.O. (2000). Public health law: Power, duty, restraint. Berkeley: University of California Press.
Haddad, L. M., & Geiger, R. A. (2022). Nursing ethical considerations. In StatPearls. StatPearls Publishing. www.ncbi.nlm.nih.gov/books/NBK526054/
Hochbaum, G. M. (1958). Public participation in medical screening programs: A socio-psychological study. United States. Public Health Service. Division of Special Health Services./z-wcorg/
Institute of Medicine (US) Committee on Assuring the Health of the Public in the 21st Century. (2002). Chapter 3. The governmental public health infrastructure. In The future of the public’s health in the 21st century. National Academies Press. www.ncbi.nlm.nih.gov/books/NBK221231/
Joszt, L. (2018, July 20). 5 Vulnerable populations in healthcare. AJMC. www.ajmc.com/view/5-vulnerable-populations-in-healthcare
Kisling, L. A., & M Das, J. (2023). Prevention strategies. In StatPearls. StatPearls Publishing. www.ncbi.nlm.nih.gov/books/NBK537222/
Marcus, B. H., & Owen, N. (1992). Motivational readiness, self-efficacy and decision-making for exercise. Journal of Applied Social Psychology, 22(1), 3–16. https://doi.org/10.1111/j.1559-1816.1992.tb01518.x
Martin, L. W., Prisco, L. C., Martinez-Prat, L., Mahler, M., & Sparks, J. A. (2021). Health risk assessment and family history: Toward disease prevention. In M. Mahler (Ed.), Precision medicine and artificial intelligence (pp. 215–236). Academic Press. https://doi.org/10.1016/B978-0-12-820239-5.00013-9
Miller, G., Roehrig, C, & Russo, P. (2015, December 10). A Framework for assessing the value of investments in nonclinical prevention. Preventing Chronic Disease, 12, 150363. https://doi.org/10.5888/pcd12.150363
Missouri Department of Health & Senior Services. (2022). Role of public health nurses. https://health.mo.gov/living/lpha/phnursing/phnroles.php
National Association of County and City Health Officials. (2017). Local health departments impact our lives every day. www.naccho.org/uploads/downloadable-resources/transition-appendix-A-Infographic.pdf
Ni, Y., Wen, Y., Bao, Y., Xu, Y., Chen, Z., Yang, X., He, J., & You, G. (2022, September 26). Nurses’ perspectives on the barriers to and facilitators of the implementation of secondary prevention for people with coronary heart disease: A qualitative descriptive study. BMJ Open, 12(9), e063029. https://bmjopen.bmj.com/content/12/9/e063029
Office of Disease Prevention and Health Promotion. (2022a). Healthy People 2030. https://health.gov/healthypeople
Office of Disease Prevention and Health Promotion. (2022b). Healthy People 2030 framework. https://health.gov/healthypeople/about/healthy-people-2030-framework
Pope, B., Hough, M. C., & Chase, S. (2016). Ethics in community nursing. Online Journal of Health Ethics, 12(2). https://doi.org/10.18785/ojhe.1202.03
Powers, M., & Faden, R. (2008). Social justice: The moral foundations of public health and health policy. Oxford University Press./z-wcorg/
Prochaska, J. O., & DiClemente, C. C. (1982). Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: Theory, Research & Practice, 19(3), 276.
Prochaska, J. O., & DiClemente, C. C. (1984). The transtheoretical approach: Crossing traditional boundaries of therapy. Dow Jones-Irwin Dorsey Professional Books./z-wcorg/
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change. Applications to addictive behaviors. The American Psychologist, 47(9), 1102–1114. https://doi.org/10.1037//0003-066x.47.9.1102
Rosenstock, I. M. (1960). What research in motivation suggests for public health. American Journal of Public Health and the Nation’s Health, 50(3 Pt. 1), 295–302.
Rosenstock, I. M. (1966). Why people use health services. The Milbank Memorial Fund Quarterly, 44(3 Suppl.), 94–127.
Rosenstock, I. M. (1990). The health belief model: Explaining health behavior through expectancies. In Health behavior and health education: Theory, research, and practice (pp. 39–62). Jossey-Bass/Wiley.
Tesser, CD. (2017, December 4). Why is quaternary prevention important in prevention? Revista de Saúde Pública, 51, 116. https://doi.org/10.11606/S1518-8787.2017051000041
Toney-Butler, T. J., & Thayer, J. M. (2022). Nursing process. In StatPearls. StatPearls Publishing. www.ncbi.nlm.nih.gov/books/NBK499937/
U.S. Department of Health & Human Services. (1999). Chapter 6. Understanding and promoting physical activity. In Physical activity and health: A report of the surgeon general. www.cdc.gov/nccdphp/sgr/chap6.htm
Vellone, E. (2016). Nursing science and prevention. Biomedicine & Prevention, vol. 0 – (37) –. https://doi.org/10.19252/000000025
Villa, G., Pennestrì, F., Rosa, D., Giannetta, N., Sala, R., Mordacci, R., & Manara, D. F. (2021). Moral distress in community and hospital settings for the care of elderly people. A grounded theory qualitative study. Healthcare, 9(10), 1307. https://doi.org/10.3390/healthcare9101307
Vollman, A. (2004). Ethics and advocacy in community practice. In A. Vollman, E. Anderson, & J. McFarlane (Eds.), Canadian community as partner (pp. 106–123). Lippincott, Williams, & Wilkins.
Waisel, D. B. (2013). Vulnerable populations in healthcare. Current Opinion in Anaesthesiology, 26(2), 186–192. https://doi.org/10.1097/ACO.0b013e32835e8c17
World Health Organization. (n.d.). Health promotion and disease prevention through population-based interventions, including action to address social determinants and health inequity. http://www.emro.who.int/about-who/public-health-functions/health-promotion-disease-prevention.html
World Health Organization. (1986). Ottawa Charter for Health Promotion, 1986.
World Health Organization. (2022). Closing the gap in a generation: Health equity through action on the social determinants of health—Final report of the commission on social determinants of health. www.who.int/publications-detail-redirect/WHO-IER-CSDH-08.1
