
Chapter Eight: Emergency Preparedness
Overview
A disaster is an event that can be human-made or environmental (or a combination of both) that causes suffering and demands more resources to manage than the community can provide. Disaster preparedness includes planning and anticipating all forms of hazards and establishing protocols for management in an ever-changing environment. Social vulnerability refers to the potential negative effects on communities caused by external stresses on human health. Such stresses include natural or human-caused disasters or disease outbreaks. Reducing social vulnerability can decrease both human suffering and economic loss.
Learning Objectives
- Discuss the disaster management cycle
- Understand the role of the community health nurse in disaster management
- Identify agents of bioterrorism and their route of delivery
Key Terms
- syndromic surveillance
- bioterrorism
Content for this chapter was adapted from “Emergency Preparedness and Response” from the Centers for Disease Control and Prevention (2024).
Introduction
Emergency preparedness and response is a key role for all nurses (American Nurses Association [ANA], 2022). Many states now require registered nurses to serve as emergency first responders in emergency departments. Public health nurses are involved in helping individuals and communities prepare for emergencies and natural disasters such as hurricanes and floods. Public health nurses also work with cities and states to assist in preparedness and recovery plans. Since public health nurses are familiar with the characteristics of different communities, the principles of preparedness, and person-centered planning for recovery, they are key members of disaster response and recovery teams. Nurses can gain specialization in National Healthcare Disaster Certification through the American Nurses Association (ANA, 2022).
Disaster Management Cycle
The terms emergency and disaster often are used interchangeably. This common use of terms can be confusing. It is easiest to understand an emergency and a disaster as being at two ends of a scale in which the size of an incident and the resources to deal with the incident are matched to varying degrees.
At one end of the spectrum, emergencies are usually small-scale, localized incidents that are resolved quickly using local resources. However, small-scale emergencies can escalate into disasters when there has been inadequate planning, inadequate resources, or wasteful use of resources. Resource management is one aspect of emergency management.
At the other end of the spectrum, disasters are typically large-scale and cross geographic, political, and academic boundaries. Disasters require a level of response and recovery greater than local communities can provide (Federal Emergency Management Agency [FEMA], 2022).
Hazard is another term often used interchangeably with disasters. It is important to note that a hazard includes acts of nature as well as human-contrived events, but a hazard cannot become a disaster unless the community or population is left vulnerable.
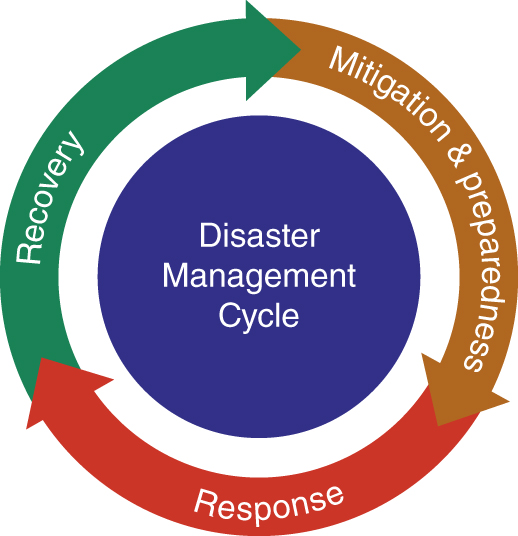
Protection from hazards includes safety consciousness in addition to disaster preparedness. The “all hazards” approach to disaster preparedness includes proactive measures to help communities plan, prepare, educate, respond, and recover from disasters (Martin et al., 2011). Managing disasters can be organized into mitigation and preparedness, response, and recover, or the disaster management cycle (Figure 8.1).
Disaster Prevention (Mitigation)
The prevention phase includes actions taken to prevent or reduce the cause, impact, and consequences of disasters. Public health nurses work with city and state planners to examine local opportunities for mitigating disasters. Examples of hazard mitigation include:
- Tying down homes or barns with ground anchors to withstand wind damage
- Digging water channels to redirect water and planting vegetation to absorb water
- Constructing levees or permanent barriers to control flooding
- Reinforcing fencing to prevent animal escapes
Disaster Preparedness
The preparedness phase includes planning, preparing, and providing educational activities for events that cannot be mitigated. Public health nurses are involved in all stages of disaster preparedness in the community and with partner agencies. The ANA has issued a position statement on the role of nurses in the event of a disaster. This document guides nurses and employers on how to release nurses to serve in emergency response situations. The entire document is available here: American Nurses Association (2002). Registered nurses’ rights and responsibilities related to work release during a disaster.
Community-wide disaster preparedness examples include these activities:
- Developing and educating community members on disaster preparedness plans for what to do, where to go, or whom to call for help in a disaster
- Exercising plans through drills, tabletop exercises, and full-scale exercises
- Creating a supply list of items that are useful in a disaster
- Walking around a farm and identifying vulnerabilities to high winds
- Working with agencies like food banks and Meals on Wheels to provide additional emergency provisions to vulnerable populations during months of the year when increased extreme weather is more likely to occur.
Disaster Response
The response phase occurs in the immediate aftermath of a disaster. During the response phase, businesses and other operations do not function normally. Personal safety and well-being in an emergency and the response phase’s duration depend on the preparedness level. Examples of response activities include:
- Implementing disaster response plans
- Conducting search and rescue missions
- Taking actions to protect yourself, your family, your animals, and others
- Addressing public perceptions about food safety
Community health nurses may engage in the care of individuals or work with partner agencies to distribute resources.
Public health nurses should be familiarized with FEMA’s Incident Command System (ICS), which organizes lines of communications and establishes clear roles and responsibilities during emergency response. Public health nurses should participate in the free educational resources provided through the FEMA website: FEMA, Emergency Management Institute, Independent Study (IS), Course List
Disaster Recovery
Restoration efforts occur concurrently with regular operations and activities during the recovery period. The recovery period from a disaster can be prolonged. Examples of recovery activities include:
- Preventing or reducing stress-related illnesses and excessive financial burdens
- Rebuilding damaged structures based on advanced knowledge obtained from the preceding disaster
- Reducing vulnerability to future disasters
Community nurses can offer trauma-informed care to affected individuals and groups (FEMA, 2022).
Six Phases of a Disaster
Communities often experience commonalities as they go through disasters. Figure 8.2 depicts the six common phases. Public health nurses need to familiarize themselves with shared responses from community members to improve their ability to provide therapeutic trauma-informed care.
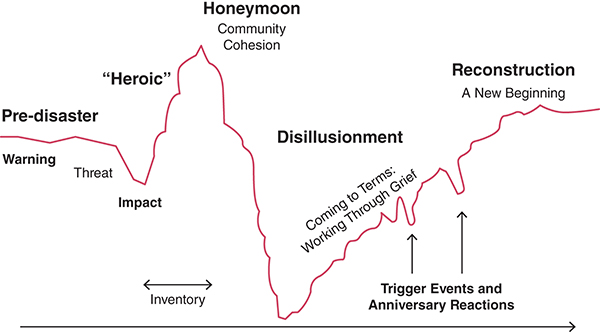
Long Description for Figure 8.2
The line begins with the pre-disaster phase, with warning and threat before the disaster impacts. The curve rises during the heroic phase and peaks at the honeymoon phase, marked by community cohesion. It then drops into disillusionment, where people work through grief. The dips as the curve rises are labeled trigger events and anniversary reactions. The curve gradually rises to the reconstruction phase, representing a new beginning.
Bioterrorism
A biological attack, or bioterrorism, is the deliberate release of viruses, bacteria, or other germs (agents) used to cause illness or death in people, animals, or plants. These agents are typically found in nature but could be changed to increase their ability to cause disease, make them resistant to current medicines, or increase their ability to be spread into the environment. Biological agents can spread through the air, water, or food. Terrorists may use biological agents because they can be extremely difficult to detect and do not cause illness for several hours to several days. Some bioterrorism agents, like the smallpox virus, can be spread from person to person; some, like anthrax, cannot.
Syndromic Surveillance
In the chapter about epidemiology, the topic of case surveillance was introduced. The methods used in case surveillance were applied to an early detection system called syndromic surveillance. Syndromic surveillance provides public health officials with a timely system for detecting, understanding, and monitoring health events. By tracking symptoms of patients in emergency departments—before a diagnosis is confirmed—public health departments can detect unusual levels of illness to determine whether a response is warranted. Syndromic surveillance was developed as a way to detect potential bioterrorism events early but has been applied to many other conditions (Henning, 2004).
Syndromic data can serve as an early warning system for public health concerns such as influenza outbreaks and has been used in responses to opioid overdoses, lung injury associated with e-cigarette or vaping product use, Zika virus infection, and natural disasters.
The National Syndromic Surveillance Program
The National Syndromic Surveillance Program collects, analyzes, and shares electronic patient encounter data received from emergency departments, urgent and ambulatory care centers, inpatient health care settings, and laboratories. Data are then integrated into a national shared platform that allows community health departments to further analyze data. Public health officials use these data in a timely and actionable manner to detect, characterize, monitor, and respond to events of public health concern. Data are detected and sent to a “Bio-Sense” platform housed by the Centers for Disease Control and Prevention (CDC). Read more about the Biosense system on the CDC website.
Agents of Bioterrorism
Bioterrorism agents can be separated into three categories, depending on how easily they can be spread and the severity of illness or death they cause. Category A agents are considered the highest risk, and Category C agents are those that are considered emerging threats for disease.
Category A
These high-priority agents include organisms or toxins that pose the highest risk to the public and national security because they can easily be spread or transmitted from person to person. Category A agents:
- Can result in high death rates and have the potential for major public health impact
- Might cause public panic and social disruption
- Require special action for public health preparedness
Examples of Category A agents include:
- Smallpox
- Botulism
- Anthrax
- Tularemia
- Viral hemorrhagic fevers (Ebola, Lassa)
- Bubonic plague
Category B
These agents are the second-highest priority because they are moderately easy to spread. Category B agents:
- Can result in moderate illness rates and low death rates
- Require specific enhancements of CDC’s laboratory capacity and enhanced disease monitoring
Examples of Category B agents include:
- Typhus fever
- Ricin toxin
- Diarrheagenic E. coli
- West Nile virus
Category C
These third-highest priority agents include emerging pathogens that could be engineered for mass spread in the future because they are easily available.
Category C agents:
- Are easily produced and spread
- Have the potential for high morbidity and mortality rates
- May have major health impact
Examples of Category C agents include:
- Hantavirus
- Influenza virus
- Tuberculosis
- Rabies virus (CDC, 2006)
Delivery Mechanisms for Biological Agents
The delivery of biological agents as a means of bioterrorism can occur in the following ways:
- Direct contact (subcutaneous anthrax)
- Simple dispersal device (airborne, nuclear)
- Water and food contamination
- Droplet or blood contact
Recognition of a Bioterrorism Event
Warnings signs of a bioterrorism event:
- Rapidly increasing disease incidence throughout the community
- A disease that is occurring in an unusual area
- An endemic occurring at an unusual time
- A large number of people dying rapidly with similar presenting manifestations
- An unusual number of dead or dying animals
- The unusual presence of liquids, vapors, or odors
A public health emergency following the deliberate or unintentional release of biological agents will require a coordinated response among public health authorities, health care providers and facilities, veterinarians, and community leaders.
Bioterrorism and Community Health
Community health nurses play a pivotal role in ensuring that state and local public health systems are prepared for public health emergencies. The nurse must be ready to respond effectively, whether it is an infectious, occupational, or environmental incident.
Accurate and timely communication with different audiences will support a successful response to bioterrorism incidents. Along with its federal partners, the CDC will communicate about national-level efforts and will assist state and local efforts. State and local public health authorities will be responsible for communicating to people within their jurisdictions about the response efforts that affect them.
The Nurse’s Role in Disaster Management
Risk Assessment
Community health assessment, also known as community health needs assessment, is a state, tribal, local, or territorial health assessment that identifies key health needs and issues through systematic, comprehensive data collection and analysis.
A community health improvement plan is a long-term, systematic effort to address public health problems based on the results of community health assessment activities and the community health improvement process.
A community health assessment gives organizations comprehensive information about the community’s current health status, needs, and issues. In turn, this information can help with developing a community health improvement plan by justifying how and where resources should be allocated to best meet community needs (CDC, 2018).
Disaster Planning
A community health assessment gives organizations comprehensive information about the community’s current health status, needs, and issues. This information can help planners develop a community health improvement plan by justifying how and where resources should be allocated to best meet community needs before disaster strikes.
Community health assessments benefits include:
- Improved organizational and community coordination and collaboration
- Increased knowledge about public health and the interconnectedness of activities
- Strengthened partnerships within state and local public health systems
- Identified strengths and weaknesses to address in quality improvement efforts
- Baselines on performance to use in preparing for accreditation
- Benchmarks for public health practice improvements (CDC, 2019)
Disaster Response and Recovery
Successful response and recovery depend on all disaster response team members having a clear understanding of pre- and postdisaster roles and responsibilities. Clearly defined roles and responsibilities are a foundation for the unity of effort among all recovery partners to jointly identify opportunities, foster partnerships, and optimize resources.
The local government and the public health department play a primary role in planning and managing all aspects of the community’s recovery. Individuals, families, and businesses look to local governments to articulate their recovery needs (FEMA, 2020).
Postdisaster nursing roles may include the following:
- Participating in damage and impact assessments with other recovery partners
- Ensuring inclusiveness in the community recovery process, including persons with disabilities and limited English proficiency
- Communicating recovery priorities to state and federal governments and other recovery stakeholders and supporters
- Incorporating critical mitigation, resilience, sustainability, and accessibility-building measures into the recovery plans and efforts
- Working closely with the recovery leadership at all levels to ensure a well-coordinated, timely, and well-executed recovery (FEMA, 2020)
Evaluation of Disaster Response
Evaluation can happen in many forms but should focus on the area, effect, and level of disaster. Ongoing assessments and surveillance reports should be completed and passed along to local governments. Disaster response teams should be evaluated for efficiency and response time. Additionally, the recovery of community services such as electricity and running potable water should be evaluated for the impact and interruption of their services.
Practice Application
➔ Setting the Scene
Glanders is a disease that usually affects livestock and farm animals and household pets, including these:
- Horses, donkeys, and mules
- Goats
- Dogs
- Cats
- Rabbits
- Guinea pigs
- Hamsters
Of note, cattle, swine, and chickens appear to be resistant to glanders. While the disease still occurs in certain parts of the world, no animal in the United States has gotten sick with glanders since the 1940s. So, it is extremely unlikely that pets or livestock in the United States will get the disease naturally.
Though not common, people have contracted glanders from sick animals. It can be a serious illness, and most people sick with glanders need to be hospitalized for treatment. As many as nine of every 10 people who contract the disease die if they do not receive specific antibiotics, while up to five of 10 people die with the correct antibiotics. Even after they are well enough to go home, people who have had glanders need to take antibiotics for several months to ensure the germs are eradicated in the body and to prevent the disease from coming back.
It can also be difficult to diagnose glanders quickly because its symptoms are the same as more common diseases like community-acquired pneumonia, influenza, or tuberculosis. In the entire world, only a few people are diagnosed with glanders each year. Because glanders in humans is so rare, most doctors are unfamiliar with the disease.
The germs that cause glanders, the bacteria Burkholderia mallei, have previously been used as a biological weapon during war, and there remains a possibility that they may again be used for a similar purpose. The germs that cause glanders are prime candidates for bioterrorism because of the combined severity and rarity of the disease.
A bioterrorism attack that releases glanders germs into the air, water, or food supply might put many people at risk of getting sick. For example, if the germs that cause glanders were released into the air in a crowded place, many people might inhale them. Or, if the germs were put into food, people who eat the contaminated food would eat the germs too. Anyone who comes into contact with these germs is in danger of getting sick with glanders. Discovering that an attack occurred may be delayed because people cannot see, smell, or taste the germs. Instead, an occurrence will likely not be identified until doctors begin to see many people sick with fevers and respiratory illnesses. Once doctors diagnose patients with glanders, they will work with public health authorities to find out how the patients came into contact with the glanders germs.
Public health authorities study glanders and many other germs to be prepared if a bioterrorism attack ever occurs. They develop bioterrorism response plans, which are extremely valuable and key to protection against bioterrorism attacks (CDC, 2017).
➔ Think About It
Nurses’ roles in public health emergencies vary depending on the nurses’ areas of focus. Select a community or public health nursing role from the following:
- Nurse at a public health department
- Nurse at a hospital internal medicine department
- School nurse at a middle school
- Home visiting nurse at Nurse Family Partnership, with a focus on families with children under 5 years of age
Answer these questions and then discuss your responses with classmates who have selected the same or different roles:
- What category of agents of bioterrorism is glanders?
- What is your role in preparing for a disaster like glanders in the community? In the workplace?
- What steps would you take if you suspect a patient has glanders or another disease that may be used in a bioterrorism attack?
- What is your role in each step of the disaster management cycle for outbreaks such as the one described in the case study?
- How willing are you to respond during an outbreak when there are unknown levels of risk?
Additional Resources
CDC – Emergency Preparedness and Response
CDC, Emergency Preparedness and Response – Bioterrorism
Ready (National public service campaign to educate and empower disaster response)
References
American Nurses Association. (2022). Disaster preparedness. www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/
Centers for Disease Control and Prevention. (2006). Bioterrorism overview. https://emergency.cdc.gov/bioterrorism/pdf/bioterrorism_overview.pdf
Centers for Disease Control and Prevention. (2017). Glanders. https://web.archive.org/web/20231128200831/https://www.cdc.gov/glanders/bioterrorism/threat.html
Centers for Disease Control and Prevention. (2018). Community health assessment. www.cdc.gov/publichealthgateway/cha/index.html
Centers for Disease Control and Prevention. (2019). Community health assessments & health improvement plans. www.cdc.gov/publichealthgateway/cha/plan.html
Centers for Disease Control and Prevention. (2024, March 1). Emergency preparedness and response. https://www.emergency.cdc.gov/
Federal Emergency Management Agency. (2020). Local disaster recovery managers responsibilities. www.fema.gov/emergency-managers/national-preparedness/frameworks/community-recovery-management-toolkit/recovery-planning/local-disaster-recovery-managers-responsibilities
Federal Emergency Management Agency. (2022). https://www.fema.gov/
Federal Emergency Management Agency & Substance Abuse and Mental Health Services Administration. (2023). Crisis counseling assistance and training program guidance: CCP application toolkit, version 5.3. https://www.samhsa.gov/sites/default/files/dtac/ccptoolkit/fema-ccp-guidance.pdf
Henning, K. J. (2004). Overview of syndromic surveillance: What is syndromic surveillance? www.cdc.gov/mmwr/preview/mmwrhtml/su5301a3.htm
Martin, M. L., Jenkins, H. A., Mehring, B. B., & Ma, A. C. (2011, Spring/Summer). All hazards, all communities: An approach to disaster preparedness and policy. The Journal of Race and Policy, 7(1), 26–39.
Romão, X., & Pereira, F. L. (2022). Smart disaster risk reduction and emergency management in the built environment. In M. Bolpagni, R. Gavina, & D. Ribeiro (Eds.), Industry 4.0 for the built environment: Methodologies, technologies and skills (pp. 315–340). Springer International Publishing. https://doi.org/10.1007/978-3-030-82430-3_14
