
Chapter Eleven: Current Topics
Overview
Community health nurses play a vital role in the communities they serve as advocates for patients and members of the community as they negotiate the health impact of pressing current issues. This chapter provides a brief overview of four of the issues facing nurses and the communities they serve.
Key Terms
Opioid use Disorder
Substance use disorder (SUD) occurs when the recurrent use of alcohol and/or drugs causes clinically significant impairment, including health problems, disability, and failure to meet major responsibilities at work, school, or home. Opioid use disorder is one type of SUD. The terms opiate and opioid are often used interchangeably, but there are differences between the two. Opiates are a class of drugs naturally found in the opium poppy plant and include the drugs morphine and codeine; these are referred to as “natural opioids.” The term opioid is a broader term and encompasses all substances natural or synthetic (derived in a laboratory) that bind to the receptors in the brain. This includes the naturally derived opiates (morphine) as well as synthetic (fentanyl) and semi-synthetic (natural and laboratory) opioids like oxycodone. Opioids are used to treat pain because they block pain signals between the brain and the body. Opioids were originally prescribed for cancer pain. Heroin, a street drug, is also a natural opiate. In addition to providing pain relief, opioids make some people feel relaxed and high (Butanis, 2022).
Since 1999, more than 932,000 people have died from a drug overdose. In 2020 alone, nearly 92,000 people died from a drug overdose, and over 68,000 or 75% of these deaths involved an opioid overdose (Centers for Disease Control and Prevention [CDC], 2022f). In 2020, an average of four Virginians died every day from an opioid overdose (Virginia Department of Health, 2021).
The Opioid Epidemic
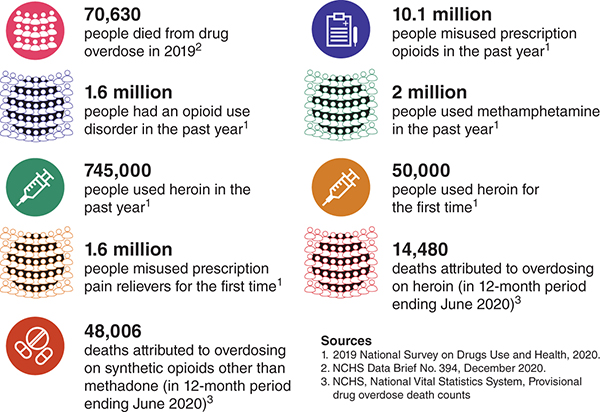
Figure 11.1: The Opioid Epidemic by the Numbers (Adapted from U.S. Department of Health and Human Services Digital Communications Division, 2022)
Long Description for Figure 11.1
70,630 people died from drug overdose in 2019. 1.6 million people had an opioid use disorder in the past year. 745,000 people used heroin in the past year. 1.6 million people misused prescription pain relievers for the first time. 48,006 deaths attributed to overdosing on synthetic opioids other than methadone, in 12-month period ending June 2020. 10.1 million people misused prescription opioids in the past year. 2 million people used methamphetamine in the past year. 50,000 people used heroin for the first time. 14,480 deaths attributed to overdosing on heroin, in 12-months period ending June 2020. Sources: 1, 2019 National Survey on Drugs Use and Health, 2020. 2, N C H S Data Brief Number 394, December 2020. 3, N C H S, National Vital Statistics System, Provisional drug overdose death counts.
In the late 1990s, pharmaceutical companies used aggressive marketing to encourage providers to prescribe opioids to patients for pain relief. The companies assured the providers that patients would not become addicted to opioid pain relievers, leading to increased prescribing rates and widespread misuse of prescription and nonprescription opioids. It then became clear that these medications were in fact highly addictive, with dependency leading to an increase in opioid overdose deaths in 1999, primarily related to prescription opioid overdoses (CDC, 2022f; see Figures 11.1 and 11.2).
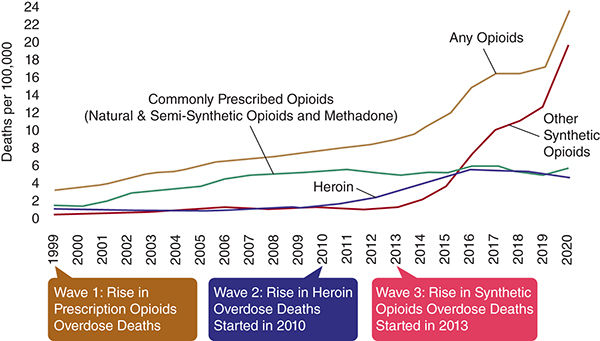
Long Description for Figure 11.2
The y-axis measures deaths per 100,000 with values ranging from 0 to 24. The x-axis lists the years from 1999 to 2020. Any opioid: Deaths increased from 4 to 24 from 1999 to 2020. Heroin: Deaths increase gradually from 2 to 6 from 2010 to 2020. Commonly prescribed opioids, natural, semi-synthetic opioids, and methadone: Deaths increased from 2 to 6 from 1999 to 2020. Other synthetic opioids: Deaths increased significantly from 0 to 20 from 2013 to 2020. The first wave began in 1999 marked by a rise in prescription opioids overdose deaths. The second wave began in 2010, marked by an increase in heroin overdose deaths. The third wave started in 2013, showing a sharp rise in deaths from synthetic opioids overdose. All data are approximate.
By 2010, many people who had been prescribed opioids were dependent on them; however, providers were no longer readily prescribing them, so people were turning to heroin to get the same feeling. When people are dependent on or addicted to opioids, they need them to function in everyday life. If they do not take the opioids, they experience withdrawal symptoms that include but are not limited to nausea, vomiting, diarrhea, abdominal cramping, excessive sweating, runny nose, and muscle aches (CDC, 2022f).
By 2013, there was an increase in synthetic opioid overdoses from illicitly manufactured fentanyl. Fentanyl is 50 to 100 times more potent than heroin and is often cut with heroin (CDC, 2022f).
In 2017, the U.S. Department of Health and Human Services declared the opioid crisis a public health emergency (Assistant Secretary of Public Affairs, 2017). In late 2020, Purdue Pharma, one of the drug companies that encouraged providers to prescribe opioids, pleaded guilty to impeding the U.S. drug enforcement efforts to combat the addiction crisis (Mulvihill, 2020).
Affected Populations
No part of the United States is unaffected by the opioid epidemic. Additionally, all races, ethnicities, and ages are affected by the opioid epidemic (Table 11.1). This open educational resource focuses on the state of Virginia and the United States. However, the Kaiser Family Foundation (KFF) provides statistics for all states. In the United States and the state of Virginia, KFF found that the majority of opioid overdoses were among White non-Hispanics, followed by Black non-Hispanics. Further, the majority of opioid overdose deaths occurred in people between the ages of 25 and 44 (Figure 11.3).
|
Location |
White Non-Hispanic |
Black Non-Hispanic |
Hispanic |
Other |
|---|---|---|---|---|
|
United States |
69% |
17% |
12% |
2% |
|
Virginia |
67% |
26% |
4% |
1% |
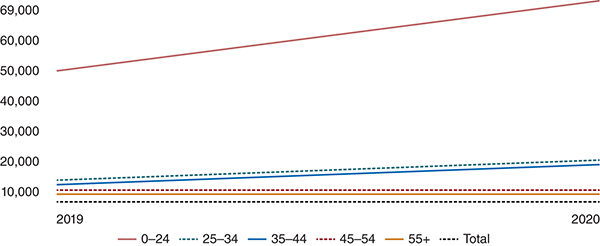
Long Description for Figure 11.3
The y-axis measures the number of deaths ranging from 10,000 to 69,000. The x-axis lists the years. The approximate data are as follows. Age group 0–24 shows a gradual increase from 50,000 to 69,000 from 2019 to 2020. Age groups 25–34 and 35 to 44 show a slight increase. Age groups 45–54 and 55 plus and total show no significant increase. All data are approximate.
Prescription drug monitoring programs are a way for providers to check whether a person has recently received a prescription for a controlled substance. This electronic database tracks controlled substance prescriptions in a state. Prescription drug monitoring programs can provide health authorities with timely information about prescribing and patient behaviors that contribute to the epidemic. This measure was put in place to prevent overprescribing of controlled substances (CDC, 2021b).
The overall national opioid dispensing rate declined from 2012 to 2020. In 2020, the dispensing rate had fallen to the lowest in 15 years, at 43.3 prescriptions per 100 persons. Nevertheless, dispensing rates continued to remain very high in certain areas across the country, and 3.6% of U.S. counties had enough opioid prescriptions dispensed for every person to have one (CDC, 2022e).
Research indicates that 43% of people being treated for SUD have a diagnosis or symptoms of mental illness, particularly depression and anxiety. Substance use disorder also often occurs with attention-deficit/hyperactivity disorder, psychotic illness, borderline personality disorder, antisocial personality disorder, and posttraumatic stress disorder (PTSD). Additionally, people with schizophrenia have higher rates of alcohol, tobacco, and drug use disorders than the general population (National Institute on Drug Abuse [NIDA], 2020).
There is a lot of stigma surrounding SUD. People with SUD continue to be blamed for their disease. The public, including many in health care and the justice system, continue to view SUD as a moral weakness and flawed character rather than a complex brain disorder with behavioral components. It is important to note that SUD is a chronic, relapsing disease, and stigma on the part of the health care provider can lead to substandard care or discourage people with SUD from seeking care when they need it (CDC, 2022g).
The opioid epidemic does not affect only the person who is using drugs. It also affects families and communities. Foster care placements have risen alongside the opioid epidemic, as has opioid-related neonatal abstinence. Moreover, premature deaths cause family members and communities to lose out on benefits from an individual’s lifetime earnings; there are added health care costs from health care complications caused by drug use (e.g., hepatitis) and added costs from criminal justice expenses. Furthermore, there is a loss of productivity and reduced quality of life as a result of drug use (Crowley et al., 2019; Kuehn, 2021).
Treatments
According to the CDC, the best way to prevent opioid overdose deaths is to improve opioid prescribing, reduce exposure to opioids, prevent misuse, and treat opioid use disorder (CDC, 2018). Additional treatments are explored in the next section.
Medication-Assisted Treatment
Medication-assisted treatment (MAT) is the use of medication in combination with counseling and behavior therapy to treat SUDs. Medication-assisted treatment is primarily used to treat addiction to opioids such as heroin and prescription pain relievers containing opiates. The ultimate goal of MAT is to allow people to live self-directed lives. This treatment approach has been shown to improve survival, increase retention in treatment, increase people’s ability to find and retain work, and improve birth outcomes among pregnant people with SUD. Additionally, MAT can lower a person’s risk of contracting HIV and hepatitis C (Substance Abuse and Mental Health Services Administration [SAMHSA], 2022; Kleinman & Sanches, 2023; National Academies of Sciences et al., 2019).
There are a few MAT options.
Methadone
Methadone is prescribed to reduce opioid cravings and withdrawal and blunt or block the effects of opioids. It is a synthetic opioid agonist that eliminates withdrawal symptoms and relieves drug cravings by acting on opioid receptors in the brain—the same receptors that other opioids such as heroin, morphine, and opioid pain medications activate (Figure 11.4). Methadone must be dispensed through specialized opioid treatment programs, and patients usually go to the clinic daily to get their methadone dose. Eventually, stable patients may receive take-home doses if they meet certain criteria, such as a period of time without illicit drug use. However it is important to note that methadone, like other opioids, can be associated with overdose deaths, particularly when misused such as taking it in combination with other substances, such as alcohol or benzodiazepines (NIDA, 2021).
Buprenorphine
Buprenorphine is another MAT option. It suppresses and reduces cravings for opioids. It is a partial opioid agonist, meaning that it binds to those same opioid receptors but activates them less strongly than full agonists do (Figure 11.4). It can be prescribed by more providers, including primary care providers, but there are limits to the number of patients who can be treated (NIDA, 2021).
Naloxone
Naloxone (Narcan®) is known as an opioid antagonist or “blocker.” It blocks the effects of opioids. When combined with buprenorphine, it is absorbed and activated in the body only if the drug is injected instead of being dissolved in the mouth, as prescribed. This is to discourage people from injecting Suboxone® (a trade name for buprenorphine). Naloxone is used to reverse opioid overdoses (SAMHSA, 2024; Figure 11.5).
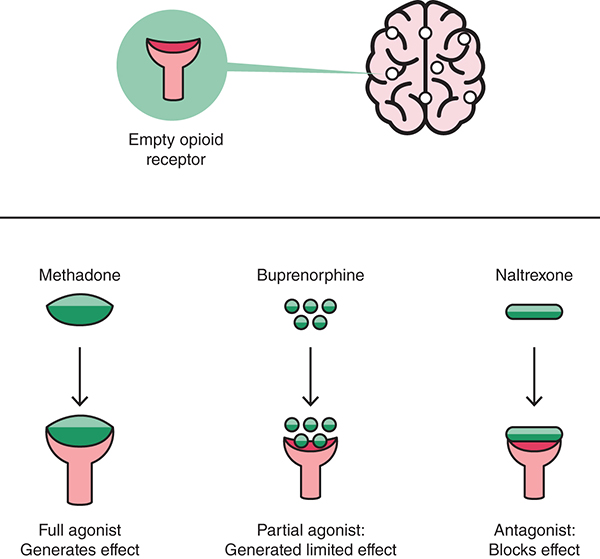
Long Description for Figure 11.5
The interaction of opioids with the empty opioid receptors is as follows. Methadone, a full agonist, binds to the empty receptor completely and generates a full effect. Buprenorphine, a partial agonist, binds to the receptor partially and generates a limited effect. Naltrexone, an antagonist, blocks the receptor, preventing any opioid effect.
Naltrexone
Naltrexone blocks the sedative effects of opioids and prevents feelings of euphoria. It is an opioid antagonist, which means that it works by blocking the activation of opioid receptors (Figure 11.4). Instead of controlling withdrawal and cravings, it treats opioid use disorder by preventing any opioid drug from producing rewarding effects such as euphoria (NIDA, 2021; SAMHSA, 2022).
Harm Reduction
Harm reduction is another strategy that is used to deal with the negative consequences of using drugs. It may or may not include MAT. Harm reduction is a form of social justice built on respect for people who use drugs as well as for the rights of people who use drugs. The social justice window “recognizes that the realities of poverty, class, racism, social isolation, past trauma, sex-based discrimination, and other social inequalities affect both people’s vulnerability to and capacity for effectively dealing with drug-related harm” (National Harm Reduction Coalition, 2020).
There is no one way to implement a harm reduction program. Generally, providers meet people where they are and determine what can be done to help them. This can include safe injection sites, primary prevention such as access to syringe exchanges to prevent the spread of HIV and hepatitis, access to providers who respect people who use drugs and treat them in a nonjudgmental manner, access to MAT, access to abstinence programs and anything that will help people who use drugs. “Drug use is a complex, multi-faceted phenomenon that encompasses a continuum of behaviors from severe use to total abstinence, and acknowledges that some ways of using drugs are clearly safer than others” (National Harm Reduction Coalition, 2020).
The Nurse’s Role in Harm Reduction
Nurses often spend a lot of time with their patients in direct clinical care as well as in education; this time is an opportunity to engage the patient in conversation about how to keep themself safe. As previously mentioned, harm reduction involves nonjudgmental patient-centered engagement. It is focused on reducing the harm of drug use to the individual and society for patients who are unable or unwilling to stop using drugs at the moment when they are interacting with you as the nurse in the health care setting. Many individuals experiencing SUD have experienced one or more traumas in their lifetime. A systematic review of American Indian and Native Alaskan substance users showed that the lifetime trauma rate varied from 21% to 98% (Herron & Venner, 2022). To learn more about practicing trauma-informed care, see Chapter Nine: Trauma-Informed Care.
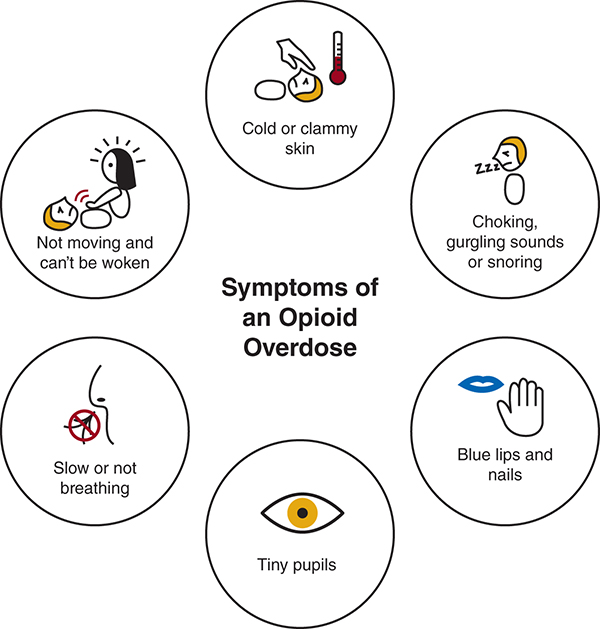
As the nurse, you are not minimizing or ignoring the harms associated with drug use but rather working to engage the individual in behaviors that reduce those harms. Patient teaching opportunities include recognizing the signs of an overdose, using fentanyl test strips, giving patients a naloxone kit, discussing safe use strategies (e.g., do not use alone, use sterile water, consider smoking or snorting rather than injecting), and syringe access services (University of Michigan Injury Center, n.d.). Nurses should be able to identify the signs and symptoms of an opioid overdose (Figure 11.6).
On a broader level, NAADAC, the association for addiction professionals, has the following suggestions for decreasing community-wide SUD (NAADAC, 2022):
Understand the issues. Nurses can learn more about state and federal policies that have an impact on how medications are prescribed and dispensed and laws that determine how and if illicit substances are controlled and criminalized. You can learn more about policy issues that affect community members and professionals through the following links:
- White House Office of National Drug Control Policy (ONDCP) (whitehouse.gov)
- Bureau of International Narcotics and Law Enforcement Affairs (INL)
- Health Resources & Services Administration (HRSA)
- National Institute on Alcohol Abuse and Alcoholism (NIAAA)
- National Institute on Drug Abuse (NIDA)
- Substance Abuse and Mental Health Services Administration (SAMHSA)
Become an advocate. As a nurse, you are a trusted professional. You can:
- Write a letter to your legislature
- Write an informed letter to your local paper aimed at helping the general public understand the issue or a current bill in the legislature
- Seek more information about how to advocate for this issue from your state nurses association like the VNA, Virginia Nurses Association
Practice Application
➔ Setting the Scene
The opioid epidemic is widespread, affecting every state in the United States. As an independent polling and public policy research company, KFF has a collection of data related to the epidemic, including information on deaths and the prevalence of opioid use disorder. The collection can be accessed at https://www.kff.org/statedata/collection/opioid-epidemic/
➔ Think About It
Using the KFF collection, look up the data for your state.
- Does the death rate from opioid overdose in your state surprise you? Why or why not?
- Which of the classifications of data (e.g., death by sex or by age) was the most surprising?
- Did your state differ from national trends in any categories? What aspects of the community might influence this difference?
- What do you think is one thing that might lessen the opioid-related death rate in your state?
Additional Resources
Virginia Department of Health – Drug Overdose and Related Health Outcomes
Reproductive Health Care
In the United States, a history of systemic inequities and injustices is reflected in the history of reproductive health care. Enslaved and immigrant women were forced to become nonconsenting research subjects for physicians to practice their gynecological techniques. Gynecological abuse continues in family planning services. Currently, threats include forced sterilization, long-acting reversible contraceptives, and threats to individual parenthood. These abuses disproportionately affect individuals who are Black, Indigenous, and people of color, those who are economically disadvantaged, those with disabilities, immigrants, the LGBTQIA+ community, and those who are incarcerated (Center for Reproductive Rights, 2022). Black and Indigenous women continue to bear a disproportionate burden of the maternal mortality rates in the United States.
Many organizations have been formed to address the legacy of these abuses. One such organization, the SisterSong Reproductive Justice Collective, was formed in 1994 in response to the discriminatory past of gynecological care within Black communities. Embracing reproductive justice as a framework, the SisterSong Reproductive Justice Collective conceptualized four basic tenets:
- The individual’s right to maintain personal bodily autonomy
- The individual’s right to have children
- The individual’s right to not have children
- The individual’s right to parent children in safe and sustainable communities (SisterSong, n.d.).
Reproductive oppression can be addressed through frameworks that address reproductive health, reproductive rights, and reproductive justice. Reproductive health ideology ensures access to reproductive health services. Reproductive rights are rooted in the concept that everyone has the right to universal legal protections. A reproductive justice framework analyzes the impact of reproductive oppression as the result of multifaceted barriers to social justice and human rights. Individuals may have limited options concerning their pregnancy outcome, which is further influenced by their race, gender, class, sexual orientation, and age. According to the TEACH Abortion Training Curriculum,
Reproductive experience occurs within a social, structural, political, environmental, and economic context, including insurance, employment, food, safe water and air, and education. Supporting reproductive justice and bodily autonomy requires that we examine, understand, and improve the structural and social context in which people experience reproduction and parenting. (Fleming et al., 2022)
Social justice, intersectionality, and contributions of Black communities are foundational to reproductive justice frameworks. In contrast, the reproductive rights movement has historically focused on the needs of cisgender White heterosexual women regarding their legal right to abortion. Reproductive justice encompasses and embraces transformational and grassroots movements led by Black and Indigenous peoples and people of color to improve institutional policies and create sustainable system changes that enhance and empower the reproductive choices and lives of historically marginalized communities. Health care providers should be aware of the impact of the devaluation of the childbearing of marginalized populations and ensure respectful care that is focused on individual autonomy and honors the patient’s preferences and values.
United States Law
In 1973, the U.S. Supreme Court decision in Roe v. Wade established that abortion was legal and state laws cannot interfere with a woman’s right to end a pregnancy. During the following 50 years, the Supreme Court superseded states as the driving force in crafting abortion policy. On June 24, 2022, the Supreme Court issued Dobbs v. Jackson Women’s Health Organization, a decision that overturned preexisting protections and sent decision-making on issues of abortion back to the states (Jung et al., 2023). Abortion laws changed quickly thereafter, and they continue to vary widely depending on each state’s political climate.[1] The position of the American Nurses Association (ANA) is that women should have full access to reproductive health care (ANA, 2022).
Increasing legislation and the resulting restrictive access to abortion care directly affect overall community health locally and nationally. One in four individuals who is pregnancy capable will seek abortion care in the United States. This includes women and non-binary and transgender individuals who experience an undesired pregnancy. Those living in restricted states with little or no access to abortion services have poorer financial and health outcomes, including higher rates of abortion-related mortality, than their counterparts in states without such restrictions (Jung et al., 2023).
Community Health and Abortion
While laws seek to ban the practice of abortion, individuals will still seek and need abortion care throughout the community. Communities with increased legal restrictions and laws regarding abortion care are associated with increased maternal morbidity and mortality. Decreased access to abortion care is associated with decreased health outcomes. In 2016, the United States had a 45% higher unintended pregnancy rate than the global average (Aztlan-James et al., 2017; Singh et al., 2010; Finer & Zolna, 2016).
Individual patient pregnancy preferences must be addressed and are an essential component within the framework of public health. Primary care and community clinics are well positioned and have an ethical responsibility to provide reproductive health screening, pregnancy options counseling, contraceptive services, miscarriage management, and appropriate referral or provision of abortion services.
The Nurse’s Role in Reproductive Health Care
Community health nurses should be committed to supporting policy solutions that ensure all people have access to a full range of preventive, reproductive, and sexual health services.
Abortion is an essential component of reproductive health care. Delivering care may present an ethical challenge to health care providers in communities where the legal status of abortion is uncertain. Stigma regarding abortion is further associated with unethical practices, including “refusal to provide abortion services to patients, alleging conscientious objection or religious directives, and discrimination against patients who may have complications of ectopic pregnancy or abortion, without tending to the obligation of preventing harm to patients for whose care they are responsible” (Fleming et al., 2022). In addition, people who seek or undergo abortion may keep their decision a secret and may not report it in their medical history, which could prove detrimental.
Medical facilities within the community must practice transparency and disclose any religious affiliation and their potential impact on health services in order to ensure that patients and health care providers can make informed decisions. Although most states allow health care professionals to refuse involvement in abortion on the basis of conscientious objection, many abortion providers characterize their provision as conscience based (Advancing New Standards in Reproduction Health, 2022).
Practice Application
➔ Setting the Scene
Frontline: The Abortion Divide
Watch this video by scanning the QR code or visiting https://www.pbs.org/wgbh/frontline/documentary/the-abortion-divide/

➔ Think About It
The Frontline video provides an overview of the fight of abortion. Drawing on the video and your experiences, answer the following questions:
- What is the criminalization of abortion?
- How does abortion access positively affect individuals who can give birth?
- What are some examples of recent legislation on reproductive rights?
- How do existing restrictive reproductive rights laws affect community health?
- How are reproductive rights connected to racial justice?
- What does it mean for the Supreme Court to overturn reproductive rights?
Additional Resources
Center for Reproductive Rights
National Organization for Women – Reproductive Rights and Justice
Gender-Affirming Care
Content for this section was adapted from “Patient-Centered Care for Transgender People: Recommended Practices for Health Care Settings” from the Centers for Disease Control and Prevention (2022c).
Gender-affirming care is a supportive form of health care. It consists of an array of services that may include medical, surgical, mental health, and nonmedical services for transgender and non-binary people (OASH/Office of Population Affairs, 2022). Many transgender people experience stigma and discrimination in their day-to-day lives that can affect access to health care. In particular, many transgender women of color (specifically those who are Black or African American and Hispanic or Latino) have reported being victims of harassment and violence, even in health care settings. Given these challenges, transgender people, especially transgender women of color, may delay seeking medical care because of fear or experience of negative treatment by health care staff.
Concepts
The term transgender has varying definitions across cultures and communities. Most describe transgender people as those who have a gender identity that is different from their sex assigned at birth. Sex assignment at birth is based on the external genitalia, whereas gender identity refers to the internal sense of one’s gender. Although people use many different terms to describe themselves, in general, a transgender woman is someone who was listed as male on their birth certificate and whose gender identity is female, and a transgender man is someone who was listed as female on their birth certificate and whose gender identity is male. Other people may have a gender identity that is fluid or non-binary; their gender is neither male nor female, nor is it a mix of male and female. Sexual orientation, which relates to emotional and sexual attraction to others, is distinct from gender identity; transgender people may have any sexual orientation regardless of their gender identity. For transgender people, the discordance between their gender identity and their assigned sex at birth can cause great distress, necessitating access to patient-centered, gender-affirming health care (CDC, 2022c).
For transgender and non-binary children and adolescents, early gender-affirming care is crucial to overall health and well-being because it allows the child or adolescent to focus on social transitions and can increase their confidence while navigating the health care system. Nurses can help families navigate resources and provide education that may empower them to have the necessary and sometimes difficult conversations within their own families and with health care providers (OASH/Office of Population Affairs, 2022).
Many but not all transgender people change their physical appearance. This is sometimes called gender affirmation. These changes can include modifications to clothing, hairstyles, and mannerisms. Many will change their first name and may want others to refer to them by pronouns that correspond to their gender identity. It is estimated that about 60%–70% of transgender people take hormones and that about 20%–40% have had one or more gender-affirming surgeries to alter their physical characteristics. Decisions about medical or surgical treatments depend on personal choice and cost. Nurses in all settings need to develop a comfort level by asking individuals to state their gender and their preferred pronouns. Information about the individual’s preferences should be integrated throughout the care continuum to ensure patient-centered care (CDC, 2022c).
Common Terms
- Cisgender: Describes a person whose gender identity aligns with their sex assigned at birth.
- Gender-diverse or expansive: An umbrella term for a person with gender identity and/or expression broader than the male or female binary. Gender minority is also used interchangeably with this term.
- Gender dysphoria: Clinically significant distress a person may feel when the sex or gender assigned at birth differs from their identity.
- Gender identity: One’s internal sense of self as man, woman, both, or neither.
- Non-binary: Describes a person who does not identify with the man or woman gender binary.
- Transgender: Describes a person whose gender identity and/or expression is different from their sex assigned at birth and societal and cultural expectations around sex. (CDC, 2022c)
How Many People Identify as Transgender?
According to recent estimates, between 0.4% and 0.6% of American adults identify as transgender. The new estimates are larger than the previous estimate from roughly a decade ago. The analyses note several reasons that may account for this difference, including a perceived increase in visibility and social acceptance of transgender people, which may increase the number of individuals willing to identify as transgender on a government survey. It is also noted that younger adults aged 18 to 24 years are more likely than older adults to say they are transgender (CDC, 2022c).
Transgender Health Needs
Studies indicate that transgender people experience multiple health disparities as a result of stigma, discrimination, and unique barriers to accessing quality care. A summary of the barriers to achieving positive health outcomes and the consequences of those barriers is presented next. The purpose of identifying these barriers is to build an understanding of the difficulties transgender people face so that health care providers can help break down barriers.
Stigma and Discrimination
The majority of transgender people experience various forms of harassment, victimization, and discrimination in their daily lives (Figure 11.7).
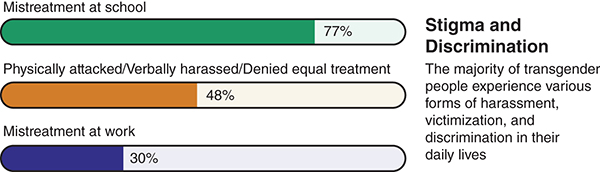
In addition to facing discrimination, transgender people are more likely than the general population to be homeless, unemployed or underemployed, and living below the federal poverty level.
The trauma and stress induced by stigma and discrimination, as well as the related effects of underemployment and unemployment, homelessness, lack of access to transition-related care, and lack of insurance, among other issues, can create a great burden on the mental and physical health of transgender people.
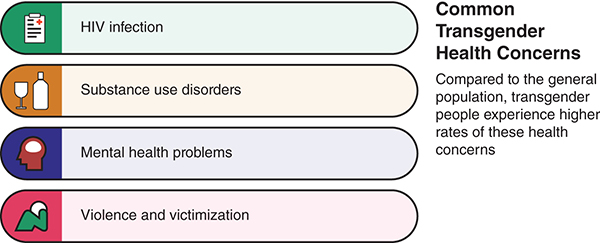
Figure 11.8 illustrates research findings from several sources, including the National Academy of Medicine and the U.S. Department of Health and Human Services’ Healthy People 2020, which found that, compared with the general population, transgender people experience higher rates of several health concerns.
More specifically, studies have found that 41% of transgender people had attempted suicide at some point in their lives and that transgender women have one of the highest prevalence rates of HIV of any group. Survival sex work—or engagement in sex work to access basic necessities such as food and shelter—increases the risk for some. Transgender women, particularly those of color, have to contend with greater vulnerability to violence.
Unfortunately, transgender women of color face bias and discrimination on several fronts. For example, an African American transgender woman may face racism, stigma, and sexism in her daily life, with negative or deadly consequences for her health.
Transgender people have been shown to have higher odds of depression and attempted suicide than nontransgender (cisgender) people. These data suggests the importance of providers screening and treating patients experiencing mental health challenges (CDC, 2022c).
Barriers to Accessing Care
Lack of Trained Providers
Because of expectations of discrimination or misunderstanding in medical settings, many transgender people avoid or delay seeing a health care provider. But even when they do access care, they have difficulty finding a provider or being referred to providers who have expertise in patient-centered care for transgender people. To facilitate care, public health nurses can develop a list of gender-affirming care providers. A national resource such as Health Coverage Guide | National Center for Transgender Equality (transequality.org) is a place to start (National Center for Transgender Equality, n.d.).
Some transgender people may seek unauthorized (sometimes referred to as “underground”) care through the internet or through friends and/or other nonmedical individuals in their social circle. They may take nonprescription and potentially dangerous hormones, get silicone injections, or have silicone implants to enhance their appearance. This can lead to a higher risk of illness and injury, further complicating health disparities. For instance, sharing needles to inject silicone or hormones may place transgender people at risk for HIV and hepatitis C.
Consider speaking with the person’s health provider about the different types of medical care the person uses, or possibly speak with the person’s friend or other nonmedical people. Consider discussing possible options for safer ways to get what the person is looking for in their health care.
Lack of Insurance
Many transgender people lack health insurance, have been denied insurance coverage for transition-related care, or denied coverage of preventive care that is not consistent with the gender their insurer has listed (e.g., coverage for a transgender woman to receive prostate exams may be denied if the patient’s gender is listed as female). Federal law does not require health insurance plans to cover transition-related care, although some states have made this a requirement.
Gender-Affirming Care and Young People
Research demonstrates that gender-affirming care improves the mental health and overall well-being of gender-diverse children and adolescents. Because gender-affirming care encompasses many facets of health care needs and support, it has been shown to increase positive outcomes for transgender and non-binary children and adolescents. Gender-affirming care is patient-centered care that treats individuals holistically, aligning their outward physical traits with their gender identity.
Gender-diverse adolescents, in particular, face significant health disparities compared with their cisgender peers. Transgender and gender non-binary adolescents are at increased risk for mental health issues, substance use, and suicide. The Trevor Project’s 2021 National Survey on LGBTQIA+ Youth Mental Health found that 52% of LGBTQIA+ youth seriously considered attempting suicide in the past year (The Trevor Project, 2021).
A safe and affirming health care environment is critical in fostering better outcomes for transgender, non-binary, and other gender-expansive children and adolescents. Medical and psychosocial gender-affirming health care practices have been demonstrated to yield lower rates of adverse mental health outcomes, build self-esteem, and improve the overall quality of life for transgender and gender-diverse youth. Familial and peer support are also crucial in fostering similarly positive outcomes for these populations. The presence of affirming support networks is critical for facilitating and arranging gender-affirming care for children and adolescents. Lack of such support can result in rejection, depression and suicide, homelessness, and other negative outcomes.
The Nurse’s Role in Gender-Affirming Care
One of the most important steps for the community health nurse in creating a welcoming environment for transgender people (and indeed all people) is to address patients using their preferred names and pronouns. For many reasons, this can be challenging in health care environments. Yet, using the wrong name or pronoun can cause embarrassment and confusion. Imagine how a transgender woman would feel if a medical assistant called into the waiting room asking for “Mr. Donald Jones” rather than “Denise Jones.” To avoid such situations, here are a few suggested systems and practices that can easily be incorporated into practice:
- Ask about gender identity on registration forms. In addition to gender identity, include fields for listed sex at birth, preferred name, and pronouns. It may also be helpful to ask for names on insurance and government-issued identification documents, if different. Enter the information into the electronic health record so all staff can access this information. This information will help staff to use proper pronouns, from the front desk staff to the provider’s office. If electronic health records are not yet in place, consider using a name-alert sticker to flag patient charts. Never refer to a person as “it.” Try to avoid using gender terms or pronouns with new patients until this information is known, whether in-person or over the phone. For example:
- Instead of “How may I help you, sir?” ask, “How may I help you?”
- Instead of “Mr. or Ms.,” use the (preferred) first and last name. In the case of writing an email, the salutation Mx. is non-binary. Mx. is pronounced like “mix.”
- Instead of “He is here for his appointment,” say, “The patient is here in the waiting room,” or “Dr. Reed’s 11:30 patient is here,” or “They are here for their appointment.”
- Ask patients how they would like to be addressed. When unsure about pronouns and names, it is acceptable to ask privately and politely, “I would like to be respectful. What name and pronouns would you like me to use?” Once a patient has given this information, staff should note it in the chart and use this name in all interactions. If it is not possible to ask what pronouns must be used, choose the pronouns that most closely match the person’s gender expression or use “they/them.” See Table 11.2 for examples of pronouns that transgender people may use.
- Apologize for mistakes. Sometimes mistakes happen, and simple apologies can go a long way. If a slip occurs, it is fine to say something like, “I apologize for using the wrong pronoun/name. I did not mean to disrespect you.”
- Consider practicing with colleagues and friends. Making changes to the way one addresses other people can be challenging. It can help to practice with colleagues (CDC, 2022c).
|
Gender Expression |
Commonly Accepted Pronouns |
||
|---|---|---|---|
|
Woman-identifying pronouns |
She |
Her |
Hers |
|
Man-identifying pronouns |
He |
Him |
His |
|
Non-binary pronouns |
Ze |
Zim |
Zirs |
|
Sie/Zie |
Hir |
Hirs |
|
|
Non-binary/Gender-neutral pronouns |
They |
Them |
Theirs |
Practice Application
➔ Setting the Scene
The City of San Francisco has distinguished itself as a national leader in addressing the needs of the transgender community. Under the leadership of Executive Director Theresa Sparks, who is transgender, the San Francisco Human Rights Commission has led various groundbreaking efforts to prevent anti-transgender violence and reduce the vast disparities faced by members of the transgender community.
One of the city’s flagship initiatives has been trans-inclusive universal health care for all residents of San Francisco, which includes all medically necessary transition-related care free of cost to transgender people, care that has limited-to-no impact on the city’s budget but would be prohibitively expensive for many individuals.
In the last year alone, San Francisco has also allocated $2 million in funding to local service providers for programs working specifically with transgender residents. These programs include an employment program that has provided training and job placement for 200 transgender people in the last couple of years, the creation of a Trans Advisory Council for the city, and an HIV prevention program aimed at eliminating HIV transmission in the transgender community by the year 2020.
The city also has programs to support transgender women of color in prison and help facilitate their reentry into society following incarceration, which, according to Sparks, has cut the recidivism rate among those who have participated in the program to about 20%, compared with a statewide average of more than 50%. San Francisco is also taking direct aim at the issues of anti-transgender street violence and domestic violence. Earlier this year, the Human Rights Commission, along with 15 other community organizations, published an LGBTQIA+ community violence assessment report and has allocated funding for implementing and tracking the report’s recommendations. The city has also started a violence prevention program for transgender Latinas, one of the city’s most marginalized groups (Human Rights Campaign, 2015).
➔ Think About It
- Does your area offer similar programs to support the health and well-being of transgender people in employment, health care, or safety? How did you locate these programs?
- As a nurse, what actions can you take to ensure that you provide safe and supportive care for transgender patients?
- In your health care practice, you have a colleague who is misgendering a patient. How do you react?
Additional Resources
American Civil Liberties Union (ACLU) – Five Things to Know About Gender-Affirming Health Care
PBS, Frontline – Growing Up Trans [Documentary]
The Trevor Project – Resources About Gender Identity
US Department of Health and Human Services, Office of Civil Rights – Sex Discrimination
Climate and Health
Content in this section was adapted from “Physical Geography and Natural Disasters” by R. Adam Dastrup (2020).
As our Earth continues to warm, climate scientists have warned of the dangers to come from climate change. Communities, including the nurses who support them, must be equipped with the knowledge and the ability to make necessary changes to the way that finite resources are managed in both an ethical and equitable way.
Nurses must recognize that there are communities and populations that bear a disproportionately larger burden of climate change, pollution, and environmental risk as a result of, but not limited to, race, ethnicity, gender, nationality, age, or ability and/or other social and economic determinants of health. These historical and existing inequities influence overall health, well-being, and quality of life.
Changes in Atmospheric Greenhouse Gas Levels
Climatic data from ice core drilling rings within coral reefs and trees, ocean and lake sediments, and other sources indicate that global temperatures rise when greenhouse gases increase in the atmosphere. When greenhouse gases decrease in the atmosphere, global temperatures fall. In 1958, the National Oceanic and Atmospheric Administration (NOAA) began measuring carbon dioxide levels in real time. Direct measurements of carbon dioxide in the atmosphere indicate that every year, the concentration of the gas increases globally every 6 months and decreases 6 months later. This mostly concerns the continents in the Northern Hemisphere, where the landmass and trees are located. During the warmer months, the trees in the Northern Hemisphere begin photosynthesizing by taking carbon dioxide out of the atmosphere and using sunlight to create chlorophyll. This causes global greenhouse gases to decrease for 6 months. When the Northern Hemisphere experiences fall and winter, the trees stop photosynthesizing and become dormant, causing global greenhouse gases to increase. However, even though carbon dioxide levels increase and decrease yearly, the global trend is that carbon dioxide levels are growing yearly. Current measurements from the National Aeronautics and Space Administration (NASA) show that carbon dioxide levels are at 413 parts per million (ppm), the highest the Earth has seen in nearly a million years (NASA, 2024a). Recently, NASA has created ultra-high-resolution computer models giving scientists a data-driven visualization of carbon dioxide as it flows around the world.
Greenhouse gas levels have varied throughout Earth’s history. For example, carbon dioxide has been present at concentrations of less than 200 ppm and at higher levels than today. However, for at least 650,000 years, carbon dioxide has never risen above 300 ppm during either glacial or interglacial periods. Natural processes (e.g., volcanic eruptions and the decay or burning of organic matter) add carbon dioxide to the atmosphere and also remove it (e.g., by absorption by plants, animal tissue, and the ocean). When plants become a form of fossil fuel, the carbon dioxide in their tissue is stored with them, removing carbon dioxide from the atmosphere (NASA, 2024a).
Our problem is that fossil fuel use has skyrocketed in the past few decades, with more people driving and industrial products releasing vast quantities of carbon dioxide into the atmosphere. Burning tropical rainforests to clear land for agriculture, a practice called slash-and-burn agriculture, also increases atmospheric carbon dioxide. Cutting down trees ensures that they can no longer remove carbon dioxide from the atmosphere. Burning the trees releases into the atmosphere all the carbon dioxide stored in the trees.
The atmosphere currently holds over 40% more carbon dioxide than it did during the Industrial Revolution. Approximately 65% of that increase has occurred since the first carbon dioxide measurements were made on Mauna Loa Volcano, Hawaii, in 1958. Carbon dioxide is a critical greenhouse gas that must be monitored because of human activity. However, other greenhouse gases are increasing as well (NASA, 2024b). The primary greenhouse gases include:
- Water vapor (36% to 70% of total): the most abundant and potent greenhouse gas on the planet and part of the hydrologic cycle
- Carbon dioxide (9% to 26% of total): released from burning fossil fuels
- Methane (4% to 9% of total): released from raising livestock, rice production, and the incomplete burning of rainforest plants
- Tropospheric ozone (3% to 7% of total): from vehicle exhaust, more than doubled since 1976. (Dastrup, 2020)
Emissions and the Health Care Industry
The health care sector accounts for approximately 10% of all greenhouse emissions (Introcaso & Vernon, 2021). Hospitals that are reimbursed by Medicare and Medicaid are legally required to meet certain conditions of participation. One of the conditions mandates that hospitals develop and execute a data-driven quality assessment program, including reporting their greenhouse gas emissions. Public health nurses can partner with institutions to help them develop emission reduction plans. Some of these plans are as simple as creating systems for increasing energy efficiency by switching to LED lights, installing automatic movement-detection lighting systems that will turn off when not in use, or unplugging large equipment that is not required to stay on at all times (Introcaso & Vernon, 2021). The ANA Code of Ethics Provision 9.4 explicitly states that promoting social justice in policy extends beyond just human health and well-being. There is an ethical imperative for nurses to advocate for policies and practices that improve the natural environment (ANA, 2015). This call to action for environmental stewardship is steeped in our history as nurses, as reflected in the environmental management writings of Mary Seacole (Britannica, n.d.).
Healthy People 2030
As a direct result of climate change, exposure to harmful pollutants in the air, water, soil, food, and materials in homes and workplaces has become commonplace. More than 12 million people around the world die every year because they live or work in unhealthy environments. The community and public health nurse has an ethical commitment to actively work to achieve the goals laid out in Healthy People 2030 as related to environmental health and climate change.
Environmental pollutants can cause health problems like respiratory diseases, heart disease, and some types of cancer (Figure 11.9). Individuals with low incomes are more likely to live in polluted areas and have unsafe drinking water. Children and pregnant women are at higher risk of pollution-related health problems than are other persons (Office of Disease Prevention and Health Promotion [ODPHP], 2022).
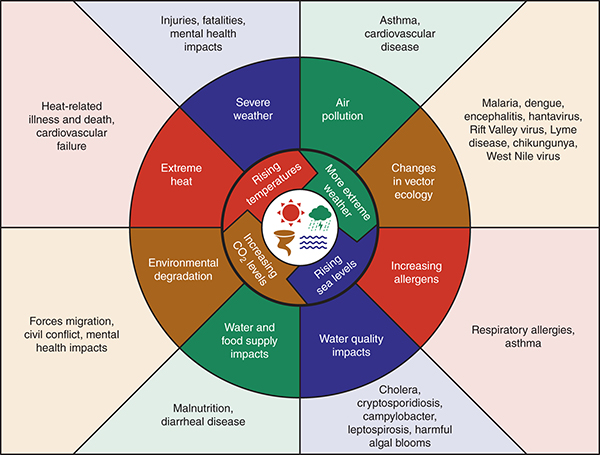
Long Description for Figure 11.9
Changes such as rising temperatures, more extreme weather, rising sea levels, and increasing carbon dioxide levels result in the following conditions. Air pollution causes asthma and cardiovascular disease. Changes in vector ecology result in malaria, dengue, encephalitis, hantavirus, Rift Valley virus, Lyme disease, chikungunya, and West Nile virus. Increasing allergens leads to respiratory allergies and asthma. Water quality impacts result in cholera, cryptosporidiosis, campylobacter, leptospirosis, and harmful algal bloom. Water and food supply impacts lead to malnutrition and diarrheal diseases. Environmental degradation causes forced migration, civil conflict, and mental health impacts. Extreme heat results in heat-related illness death and cardiovascular failure. Severe weather results in injuries, fatalities, and mental health impacts.
For the community and public health nurse, tracking environmental pollutants is key to figuring out where and how people are exposed to them. Furthermore, nurses must advocate for laws and policies to reduce different types of pollution because these will help prevent many serious health problems and deaths related to global warming.
The environmental goals of Healthy People 2030 focus on reducing people’s exposure to harmful pollutants in the air, water, soil, food, and materials in homes and workplaces. Specifically, the goals are to do the following:
- Reduce exposure to arsenic
- Reduce exposure to lead
- Reduce exposure to mercury in children
- Reduce exposure to bisphenol A (better known as BPA)
- Reduce exposure to perchlorate
- Reduce diseases and deaths related to heat
- Increase the proportion of people whose water supply meets Safe Drinking Water Act regulations (ODPHP, 2022)
The Environmental Public Health Tracking Network
This section has been modified from the “National Environmental Public Health Tracking” from the Centers for Disease Control and Prevention (2022).
Through the CDC, the Environmental Public Health Tracking Network gathers data and information needed to make decisions about our environment and health, including personal, community, regulatory, and public health decisions. The Tracking Network allows users to identify demographic factors, environmental burdens, socioeconomic conditions, and public health concerns directly related to environmental justice.
By using Tracking Network data:
- Scientists are better able to assess the connections between the environment and its effect on health.
- Public health professionals can easily assess unusual trends and events to determine which communities may be at risk.
- Elected officials can make more informed policy decisions.
- Everyone can learn more about how the environment may affect their health.
Environmental justice data tools can help users determine communities at risk, help them make informed policy decisions, and help everyone learn more about how the environment affects their health. The Tracking Network presents environmental health data in customizable maps, charts, and tables. Users can add layers to maps, including real-time data (e.g., current radar, surface smoke, active Atlantic cyclones, and transportation noise) and points of interest such as daycare centers, landfills, parks, power plants, public schools, and runways (CDC, 2022a).
What Is Climate Justice?
The nursing community must be committed to the principle that all people, regardless of race, color, national origin, or income, are entitled to equal protection from environmental and health hazards and equal access to the development, implementation, and enforcement of environmental laws, regulations, and policies. A healthy environment is a universal need and a fundamental human right. Nurses have an obligation to address health disparities and environmental injustice. Nurses recognize that climate change directly and negatively affects the most vulnerable—typically those who have done the least to contribute to the problem—and that climate justice:
- Promotes the ideology that those who have benefited the most from using fossil fuels must be dedicated to investing the same amount of success into actively reducing greenhouse gas or carbon emissions.
- Is committed to creating community action plans to address climate change and reduce greenhouse gas emissions fairly and justly.
- Requires holistic thinking. It requires listening carefully to communities that are or will be most affected by extractive industries yet are not receiving an equitable share of benefits. It requires Free, Prior, and Informed Consent before engagement with Indigenous communities. (Frierson, 2022a)
Human Impacts and Inequities
The emphasis on individual footprints has sowed discord within the environmental movement, setting what may seem to be an impossibly high bar of purity and excluding new participants.
Cultural shifts and widespread engagement are essential for enacting the scale of change we need. Projects such as community gardens and mutual aid and sharing networks can be effective at reducing consumption and fossil fuel use while building community resilience. Using less and creating more locally is a great strategy for building the climate justice movement.
When working with climate justice action, consider the hierarchy of responsibility and whether policies could be implemented that solve more than one problem at once. For example:
- How is a renter to blame for high heating emissions when the landlord controls decisions about insulation and efficiency upgrades? Can public investment fix both?
- How are workers in the fossil fuel industry to blame for extraction when they suffer severe health effects from their work? Can we provide a just transition for these laborers?
- How are industrial agricultural emissions the fault of a consumer when inadequate local or fresh food options are available in their community? How can we build food sovereignty around the world?
We also must be aware of the unequal burdens of climate change resulting from policies. One example is the flooding in historically “redlined” neighborhoods that has been documented in communities throughout the United States. Redlining was a policy implemented in the 1930s and 1940s that came out of the Home Owners Loan Corporation (HOLC). Part of the New Deal federal stimulus program, HOLC was established to provide emergency refinancing loans to homeowners, including people of color and immigrants. However, HOLC also created discriminatory housing security maps, which classified neighborhoods on the basis of their supposed “residential security.” These maps were color coded, with “A” as green, “B” as blue, “C” as yellow, and “D” as red. The “A” grade was given to wealthy neighborhoods, while the “D” grade was reserved for neighborhoods considered hazardous and home to mostly foreign-born people, socioeconomically disadvantaged White people, and Black people. Banks then used these maps to determine which neighborhoods were safe for financial investment, perpetuating racial and class inequalities. Even after the HOLC emergency funding program ended, banks continued to rely on these maps, neglecting individual borrower information. We must learn from and acknowledge HOLC’s discriminatory practices to understand how the practices affect population health even today (Bidadian et al., 2024; Conzelmann et al., 2022; Steinberg-McElroy et al., 2023; Mandal, 2023).
Neighborhoods that were redlined have features that put their residents at greater risk to experience climate change. For example, city money was far less likely to be spent on redlined neighborhoods, which means fewer trees (thus greater heat), few if any sidewalks (thus people are closer to exhaust fumes and are less safe to walk), and few parks or green spaces. These neighborhoods are more likely than others to experience flooding not only because of their location but also because of city planning that paved over areas that could previously absorb water. Compounding the problems is that the built environments are related to higher rates of chronic disease and poorer birth outcomes (Swope et al., 2022; Mandal, 2023).
Justice requires considering past harm when determining paths forward. To have restorative climate justice, it is important to measure the harms done to a given group, the lack of benefit to citizens of the extractive industries, and the parties responsible for the pollution (Frierson, 2022b).
The Nurse’s Role in Climate Justice
Climate justice actions demand the fair and meaningful involvement of all voices in addressing environmental threats. Yet, national discussions have traditionally excluded voices from marginalized communities in identifying environmental threats and practices. Nurses are well positioned to ensure that all voices are heard when developing effective, long-term solutions to bolstering human adaptation and health and safeguarding ecosystems for community survival.
Nurses are duty bound to maintain, improve, protect, and promote the health of everyone. All humans have the right to healthy and safe environments, including:
- Clean air, water, and land
- Sustainable, stable shelter
- Safe food and agricultural practices
- Products that are free from harmful chemicals
- A safe climate
- Healthy living and working conditions
- The rights and opportunities to determine the needs of one’s community and its future
Community health nurses must recognize that some communities and populations bear a disproportionately larger burden of climate change, pollution, and environmental risk. Nurses must be committed to the following principles in practice:
- Community health nurses must act with integrity, competence, diligence, and respect and in an ethical manner to ensure the equitable distribution of community resources.
- Community health nurses must exercise independent professional judgment when conducting analyses, making recommendations, taking actions, and engaging in community action plans to ensure they are fair and just.
- Community health nurses must acknowledge climate-related risks and opportunities when working with their communities in creating ongoing assessment and surveillance reports.
Without radical changes, we are facing a world of increasing inequality as climate impacts first hit those most vulnerable. Nurses and other radical thinkers can help ensure that the health impact of all the other ecological crises associated with the modern era, such as biodiversity loss, water scarcity, soil degradation, and pollution, are addressed (Frierson, 2022a).
Nurses witness firsthand the impact pollution from the transportation sector has on public health. In an August 2022 letter to the Biden administration and the U.S. Environmental Protection Agency’s administrator, Michael Regan, over 300 nurses representing 50 states and the District of Columbia called on the Agency to move forward with the next round of clean car standards for model year 2027 and beyond. The Biden administration promised to advance bold action around emissions and efficiency standards for passenger cars and trucks. According to the executive order, 50% of cars and light truck sales will be zero-emission vehicles by 2030. It is important for nurses not to become complacent but to call for continued action to ensure clean car standards are met (Cook, 2022).
Practice Application
➔ Setting the Scene
Content in this case study was adapted from the “An Inland City Prepares for a Changing Climate” in the U.S. Climate Resilience Toolkit (n.d.).
Climate adaptation and resilience were not recognized as pressing issues for the community of Blacksburg, Virginia. The current leading climate concern, the rising sea level, did not seem relevant to the city, which is located more than 300 miles from the nearest coastline. However, when Carol Davis was hired as Blacksburg’s sustainability manager, she set out to develop the town’s 2016 Climate Action Plan (pdf), which led to the town being a leader for climate resilience. The city passed its new Climate Action Plan around the same time as the Global Covenant of Mayors for Climate and Energy, a global alliance dedicated to climate leadership at the local level, was spurring communities to develop mitigation strategies to reduce greenhouse gas emissions and prepare adaptation strategies to make our communities more resilient in a changing climate. Using the plan as a starting point, Blacksburg worked to answer this charge.
Carol quickly found that best practices and tools to assess climate vulnerability, adaptation, and resilience were hard to locate for noncoastal communities. She was able to pull from three sources:
- The Climate Explorer, a visualization tool that provides graphs and maps of historical and projected climate variables for the contiguous United States at the county level
- Key findings from the Fourth National Climate Assessment (U.S. Global Change Research Program, 2018)
- The Temperate tool, which provided a concrete, guided process to help her make sense of the data and evaluate the degree to which each potential climate hazard could have an impact on an array of critical community systems
Using these tools, she determined 13 key temperature and precipitation metrics that would be most relevant to Blacksburg. Each of these metrics pointed to potential areas of vulnerability that Blacksburg might need to address.
To further explore which climate metrics might have the greatest adverse impact on the community and bring a variety of experience and expertise to the project, Carol convened the Climate Vulnerability Advisory Team, comprising experts from a variety of disciplines. The team was primarily composed of faculty from the Blacksburg-located Virginia Tech. Members of the Advisory Team provided input on invasive plants, climate trends and ecological processes, energy systems and society, surface water hydrology, extreme weather conditions, climate modeling, food system resiliency, heat stress and public health, transportation, and land use planning, stormwater engineering, climate adaptation planning, water systems and security, civil engineering, hazard mitigation planning, and forest dynamics. This team:
- Helped Carol interpret the best available climate data and modeling
- Provided critical knowledge on how those changes might specifically affect Blacksburg
- Provided input on potential adaptation policies that could help Blacksburg deal with new conditions
With these tools and the Advisory Team’s help, Carol was able to direct the project. The group focused attention on anticipated changes to climate by midcentury and end-of-century timescales, with both low- and high-emissions scenarios in mind. The group further examined the interplay between local and national geographic scopes for each of the 13 climate metrics under consideration.
In this way, the team was able to identify and prioritize the top three climate hazards of concern for Blacksburg: hotter summers, warmer winters, and increased precipitation anticipated to occur with changing precipitation patterns.
With these top climate hazards in mind, the team turned its attention to how these hazards might affect local community systems. Grouping the systems into four broad categories—People & Climate, Natural Systems, Economy & Employment, and Infrastructure & Basic Services—the team worked to identify the specific elements and systems critical to the community’s functioning and the well-being of the residents.
The team’s final assessment, the 2020 Climate Vulnerability Assessment (pdf), included plotting potential areas of vulnerability on a risk matrix to consider the degree of risk for each community system from Blacksburg’s primary climate hazards. This drew their focus to the areas of highest anticipated risk and helped them focus their efforts on potential adaptation strategies for the greatest threats. The assessment is being integrated into the town’s policy documents for future action.
➔ Think About It
- Why was having an advisory team important to the project? What benefit does having a variety of voices, experiences, and expertise bring to a study?
- An important outcome of the plan is that Blacksburg’s key decision-makers are now aware of potential areas of vulnerability and are also equipped with a list of specific actions they can take to foster short- and long-term community resilience. Imagine you are a nurse in Blacksburg. What impact (direct and indirect) would the plan have on your work? Is there any direct action you would take?
- Does your local community have a climate action plan, climate vulnerability assessment, or other climate policy? How will this affect your work?
- Are there any climate issues in your local community that will affect your work as a nurse? What steps can you take to mitigate impact through patient care?
Additional Resources
Alliance of Nurses for Healthy Environments (ANHE)
American Red Cross – Working with the Red Cross Before, During & After Disasters [Slides]
Climate for Health – Climate for Health Ambassador Training
FEMA – Individual Assistance Programs [Slides]
PBS, Frontline – Climate of Doubt [Documentary]
PBS, Frontline – Poisoned Waters | Frontline [Documentary]
TED Talk – A creative solution for the water crisis in Flint, Michigan (LaToya Ruby Frazier) [Video]
TED Talk – It’s impossible to have healthy people on a sick planet (Shweta Narayan) [Video]
TED Talk – The link between climate change, health and poverty (Cheryl Holder) [Video]
UNICEF – The impacts of climate change put almost every child at risk
UN Women – Explainer: How gender inequality and climate change are interconnected
References
Opioid Use Disorder
Assistant Secretary of Public Affairs. (2017, December 4). What is the U.S. opioid epidemic? [Text]. HHS.Gov. https://www.hhs.gov/opioids/statistics/index.html
Butanis, B. (2022). What are opioids? https://www.hopkinsmedicine.org/opioids/what-are-opioids.html
Centers for Disease Control and Prevention. (2018, April 30). Raising awareness to prevent prescription opioid overdoses. Public Health Matters. https://blogs.cdc.gov/publichealthmatters/2018/04/rxawareness/
Centers for Disease Control and Prevention. (2021b, September 9). Drug overdose: Prescription drug monitoring programs (PDMPs). https://www.cdc.gov/drugoverdose/pdmp/index.html
Centers for Disease Control and Prevention. (2022e, March 18). Drug overdose: United States dispensing rate maps [Opioids]. Overdose Prevention. https://www.cdc.gov/overdose-prevention/data-research/facts-stats/us-dispensing-rate-maps.html?CDC_AAref_Val=https://www.cdc.gov/drugoverdose/rxrate-maps/index.html
Centers for Disease Control and Prevention. (2022f, June 1). Understanding the opioid overdose epidemic. https://www.cdc.gov/overdose-prevention/about/understanding-the-opioid-overdose-epidemic.html?CDC_AAref_Val=https://www.cdc.gov/opioids/basics/epidemic.html
Centers for Disease Control and Prevention. (2022g, August 8). Stop overdose: Stigma reduction. https://www.cdc.gov/stopoverdose/stigma/index.html
Crowley, D. M., Connell, C. M., Jones, D., & Donovan, M. W. (2019). Considering the child welfare system burden from opioid misuse: Research priorities for estimating public costs. The American Journal of Managed Care, 25(13 Suppl.), S256–S263.
Herron, J. L., & Venner, K. L. (2022). A systematic review of trauma and substance use in American Indian and Alaska Native individuals: Incorporating cultural considerations. Journal of Racial and Ethnic Health Disparities. https://doi.org/10.1007/s40615-022-01250-5
Kaiser Family Foundation. (2022, May 9). Opioid overdose deaths by race/ethnicity. https://www.kff.org/other/state-indicator/opioid-overdose-deaths-by-raceethnicity/
Kleinman, R. A., & Sanches, M. (2023). Methadone-involved overdose deaths in the United States before and during the COVID-19 pandemic. Drug and Alcohol Dependence, 242, 109703. https://doi.org/10.1016/j.drugalcdep.2022.109703
Kuehn, B. M. (2021). Massive costs of the US opioid epidemic in lives and dollars. JAMA, 325(20), 2040. https://doi.org/10.1001/jama.2021.7464
Mulvihill, G. (2020). OxyContin maker Purdue Pharma pleads guilty in criminal case. AP NEWS. https://www.apnews.com/article/purdue-pharma-opioid-crisis-guilty-plea-5704ad896e964222a011f053949e0cc0
NAADAC. (2022). Advocacy. https://www.naadac.org/advocacy
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Committee on Medication-Assisted Treatment for Opioid Use Disorder; Mancher, M., & Leshner, A. I. (Eds.). (2019). The effectiveness of medication-based treatment for opioid use disorder. In Medications for opioid use disorder save lives. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK541393/
National Harm Reduction Coalition. (2020). Harm reduction principles. https://harmreduction.org/about-us/principles-of-harm-reduction/
National Institute on Drug Abuse. (2020). Part 1: The connection between substance use disorders and mental illness [Research report]. https://www.nida.nih.gov/publications/research-reports/common-comorbidities-substance-use-disorders/part-1-connection-between-substance-use-disorders-mental-illness
National Institute on Drug Abuse. (2021, April 13). How do medications to treat opioid use disorder work? https://www.nida.nih.gov/publications/research-reports/medications-to-treat-opioid-addiction/how-do-medications-to-treat-opioid-addiction-work
Pew Charitable Trusts. (2020). Medications for opioid use disorder improve patient outcomes. https://www.pewtrusts.org/en/research-and-analysis/fact-sheets/2020/12/medications-for-opioid-use-disorder-improve-patient-outcomes
Substance Abuse and Mental Health Services Administration. (2022). Medications for Substance Use Disorders. https://www.samhsa.gov/medications-substance-use-disorder
Substance Abuse and Mental Health Services Administration. (2024, March 26). Opioid overdose reversal medications (OORM). https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions/opioid-overdose-reversal-medications
University of Michigan Injury Center. (n.d.). Nurses—Harm reduction. Michigan Safer Opioid Prescribing Toolkit. Retrieved May 20, 2024, from https://injurycenter.umich.edu/opioid-overdose/michigan-safer-opioid-prescribing-toolkit/nurses/harm-reduction/
U.S. Department of Health and Human Services Digital Communications Division. (2022). Opioid facts and statistics. https://www.hhs.gov/opioids/statistics/index.html
Virginia Department of Health. (2021). Drug overdose and related health data [Opioid data]. https;//vdh.virginia.gov/opioid-data/
Reproductive Health
Advancing New Standards in Reproduction Health. (2022). The Turnaway study. University of California, ANSIRH. https://www.ansirh.org/research/ongoing/turnaway-study
American Nurses Association. (2022, March 7). Reproductive health—ANA position statement. https://www.nursingworld.org/practice-policy/nursing-excellence/official-position-statements/id/reproductive-health/
Aztlan-James, E. A., McLemore, M., & Taylor, D. (2017). Multiple unintended pregnancies in U.S. women: A systematic review. Women’s Health Issues: Official Publication of the Jacobs Institute of Women’s Health, 27(4), 407–413. https://doi.org/10.1016/j.whi.2017.02.002
Center for Reproductive Rights. (2022, August 10). Systemic racism and reproductive injustice in the United States: A report for the UN Committee on the Elimination of Racial Discrimination. https://reproductiverights.org/systemic-racism-and-reproductive-injustice-in-the-united-states/
Finer, L. B., & Zolna, M. R. (2016). Declines in unintended pregnancy in the United States, 2008–2011. The New England Journal of Medicine, 374(9), 843–852. https://doi.org/10.1056/NEJMsa1506575
Fleming, M., Shih, G., Goodman, S., & the TEACH Collaborative Working Group. (2022). TEACH abortion training curriculum (7th ed.). Bixby Center for Global Reproductive Health, University of California, San Francisco.
Jung, C., Oviedo, J., & Nippita, S. (2023). Abortion care in the United States—Current evidence and future directions. NEJM Evidence, 2(4). https://doi.org/10.1056/EVIDra2200300
Singh, S, Sedgh, G., & Hussain, R. (2010). Unintended pregnancy: Worldwide levels, trends, and outcomes. Studies in Family Planning, 41(4), 241–250.
SisterSong. (n.d.). Reproductive justice. Retrieved May 20, 2024, from https://www.sistersong.net/reproductive-justice
Gender-Affirming Care
Centers for Disease Control and Prevention. (2022c). Patient-centered care for transgender people: Recommended practices for health care settings. https://web.archive.org/web/20240507094129/https://www.cdc.gov/hiv/clinicians/transforming-health/health-care-providers/affirmative-care.html; https://www.cdc.gov/std/treatment-guidelines/trans.htm
Human Rights Campaign. (2015). Addressing anti-transgender violence: Exploring realities, challenges, and solutions for policymakers and community advocates. https://assets2.hrc.org/files/assets/resources/HRC-AntiTransgenderViolence-0519.pdf
National Center for Transgender Equality. (n.d.). Health coverage guide. Retrieved May 20, 2024, from https://www.transequality.org/health-coverage-guide
OASH/Office of Population Affairs. (2022). Gender-affirming care and young people. U.S. Department of Health and Human Services. https://opa.hhs.gov/sites/default/files/2022-03/gender-affirming-care-young-people-march-2022.pdf
The Trevor Project. (2021). 2021 National survey on LGBTQ youth mental health 2021. https://www.thetrevorproject.org/survey-2021/
Climate and Health
American Nurses Association. (2015). Code of ethics for nurses with interpretive statements./z-wcorg/.
Bidadian, B., Strager, M. P., Butler, P., & Ghadimi, H. (2024). Flood risk impacts from an unlikely source: Redlining efforts of the 1930s in Houston, Texas. Environmental Justice. https://doi.org/10.1089/env.2023.0027
Britannica. (n.d.). Mary Seacole: Jamaican nurse. In Britannica. Retrieved May 2, 2024, from https://www.britannica.com/biography/Mary-Seacole
Centers for Disease Control and Prevention. (2022a). Environmental justice. https://www.cdc.gov/nceh/tracking/topics/EnvironmentalJustice.htm
Conzelmann, C., Salazar Miranda, A., Phan, T., & Hoffman, J. (2022). Long-term effects of redlining on environmental risk exposure (SSRN Scholarly paper 4284307). https://doi.org/10.21144/wp22-09
Cook, C. (2022, August 4). Nurses call on the Biden administration to move forward with long-term cleaner car standards in 2022. Alliance of Nurses for Healthy Environments. https://envirn.org/nurses-call-on-the-biden-administration-to-move-forward-with-long-term-cleaner-car-standards-in-2022/
Dastrup, R. A. (2020). 10.6 Long-term climate change. In Physical Geography and Natural Disasters. Pressbooks. https://slcc.pressbooks.pub/physicalgeography/chapter/10-6/
Frierson, D. M. W. (2022a). Principles of environmental justice. In Climate, Justice and Energy Solutions. Pressbooks. https://uw.pressbooks.pub/climatejusticeandenergysolutions/chapter/principles-of-environmental-justice/
Frierson, D. M. W. (2022b). Who’s to blame? In Climate, Justice and Energy Solutions. Pressbooks. https://uw.pressbooks.pub/climatejusticeandenergysolutions/chapter/whos-to-blame/
Introcaso, D., & Vernon, W. (2021). Public reporting: The first step in addressing the health care industry’s bloated carbon footprint. STAT. https://www.statnews.com/2021/06/29/public-reporting-health-care-greenhouse-gas-emissions/
Mandal, A. (2023). River, race, and redlining: racialized wealth & environmental injustices along the Mississippi River. University of Minnesota Digital Conservancy. https://conservancy.umn.edu/handle/11299/254218
National Aeronautics and Space Administration. (2024a). Carbon dioxide: Latest measurement: March 2024. https://climate.nasa.gov/vital-signs/carbon-dioxide?intent=121
National Aeronautics and Space Administration. (2024b). Causes of climate change. https://science.nasa.gov/climate-change/causes
National Center for Environmental Health (2011). Impact of climate change on human health. Centers for Disease Control and Prevention. https://web.archive.org/web/20240331170936/https://www.cdc.gov/climateandhealth/effects/default.htm
Office of Disease Prevention and Health Promotion. (2022). Environmental health. Healthy People 2030. U.S. Department of Health and Human Services. https://www.health.gov/healthypeople/objectives-and-data/browse-objectives/environmental-health
Steinberg-McElroy, I., Tangtrakul, K., Alizadehtazi, B., Rosenzweig, B. R., Gurian, P. L., & Montalto, F. (2023). Associations between historical redlining and current and future exposure to stormwater flooding in New York City (SSRN Scholarly paper 4571518). https://doi.org/10.2139/ssrn.4571518
Swope, C. B., Hernández, D., & Cushing, L. J. (2022). The relationship of historical redlining with present-day neighborhood environmental and health outcomes: A scoping review and conceptual model. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 99(6), 959–983. https://doi.org/10.1007/s11524-022-00665-z
Town of Blacksburg. (2016). Town of Blacksburg: Climate action plan 2016. www.blacksburg.gov/home/showpublisheddocument?id=5773
U.S. Climate Resilience Toolkit. (n.d.) An inland city prepares for a changing climate. https://toolkit.climate.gov/case-studies/inland-city-prepares-changing-climate
U.S. Global Change Research Program. (2018). Fourth national climate assessment (pp. 1–470). https://nca2018.globalchange.gov
- This text reflects conditions as of March 2024. ↵
