
Chapter Five: Population Health
Overview
This chapter will provide an understanding of what population health is as well as what it means in the context of community and public health nursing. Population health focuses on getting available resources to the populations most in need and thus improving health outcomes. An understanding of population health can help nurses better identify issues that affect their patients, connect patients with the appropriate resources in their communities, and promote the health of vulnerable populations.
Learning Objectives
- Apply the concept of population health to nursing practice
- Understand the connections between medical care, population health, and public health strategies
- Differentiate between population health and public health
- Assess population health data and the priorities of a particular community or population
- Ascertain collaborative opportunities for individuals and organizations to improve population health
Key Terms
- population health
- public health
- health department
- health policy
- health outcomes
Introduction
The Centers for Disease Control and Prevention (CDC) defines population health as an interdisciplinary, customizable approach that allows health departments to connect practice to policy for change to happen locally (CDC, 2020). Different sectors of the community—public health, industry, academia, health care, local government entities, and many more—form nontraditional partnerships to achieve positive health outcomes. Population health “brings significant health concerns into focus and addresses ways that resources can be allocated to overcome the problems that drive poor health conditions in the population” (CDC, 2020).
Population health is slightly different from public health because public health works to protect and improve the health of communities through policy recommendations, health education and outreach, and research for disease detection and injury prevention. Public health can be defined as what “as a society [we] do collectively to assure the conditions in which people can be healthy” (Institute of Medicine, 1988). Population health, in contrast, provides “an opportunity for health care systems, agencies and organizations to work together in order to improve the health outcomes of the communities they serve” (The George Washington University, 2015).
What is Population Health?
The United States has the costliest health care system in the world, yet many countries consistently outperform the United States in terms of quality of care, health outcomes, and health expenditures. In 2008, researchers and policymakers suggested three aims that would significantly improve health care in the United States. This “Triple Aim” includes the following three goals:
- Improving the patient experience of care (including quality and satisfaction)
- Improving the health of populations
- Reducing the per capita cost of health care (Berwick et al., 2008)
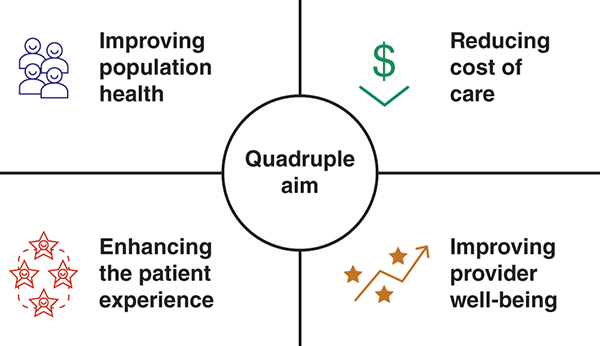
In 2014, the “Quadruple Aim”—adapted from the widely accepted Triple Aim—was suggested as a framework to optimize health care system performance (Figure 5.1). The framework encompasses reducing costs and improving population health and patient experience with a new fourth domain: promoting health care team well-being. During this time, researchers began to understand that the performance and quality pressures placed on nurses and other care team members were causing deleterious effects on their physical and mental health as well as reductions in the quality and costs of health care. Therefore, the fourth aim to improve our health system focused on provider well-being, stress reduction, burnout prevention, quality of life, and mindfulness (Arnetz et al., 2020).
Most recently, in 2022, a “Quintuple Aim” was proposed to include advancing health equity as the fifth U.S. health system improvement goal. To read more about the proposed Quintuple Aim, visit this article in the Journal of the American Medical Association (JAMA): The Quintuple Aim for Health Care Improvement A New Imperative to Advance Health Equity (Nundy et al., 2022).
To learn more about achieving health equity, see Chapter 2.
Population health focuses on preventing and managing costly, prevalent chronic diseases. The specific goals of population health are designed to achieve large-scale health improvements within neighborhoods, cities, counties, regions, or states. Population health measures target fundamental and often multiple determinants of health by addressing chronic diseases at the group level instead of the individual level. Population health evaluates current infrastructure, leverages available resources, mobilizes collective action efforts with multiple stakeholders, and through targeted actions seeks to have an impact on key health metrics such as premature death, air and water quality, tobacco use, and homelessness.
The Agency for Healthcare Research and Quality (AHRQ) defines population health as “measures that address health issues of individuals or populations defined by residence in a geographic area or a relationship to organizations that are not primarily organized to deliver or pay for health care services (such as schools or prisons)” (AHRQ, 2018). When we think of a population, we often think of a geographic area. However, in terms of population health, populations can also include people with similar characteristics, such as those who are incarcerated or people who inject drugs. For example, a public health nurse could focus their work on improving health outcomes for people who inject drugs by working to implement syringe exchanges. Figure 5.2 is a pictorial model of population health. On the left are multiple health factors (or determinants of health), and on the right, health outcomes. What is missing from this picture are people who are living healthy lives and not experiencing morbidity or early death. Also missing from this picture is causality. Causality means that one variable, such as a health factor, causes another variable, such as a health outcome, to occur. It is important to note that in some cases, variables are correlated, but one does not necessarily cause the other.
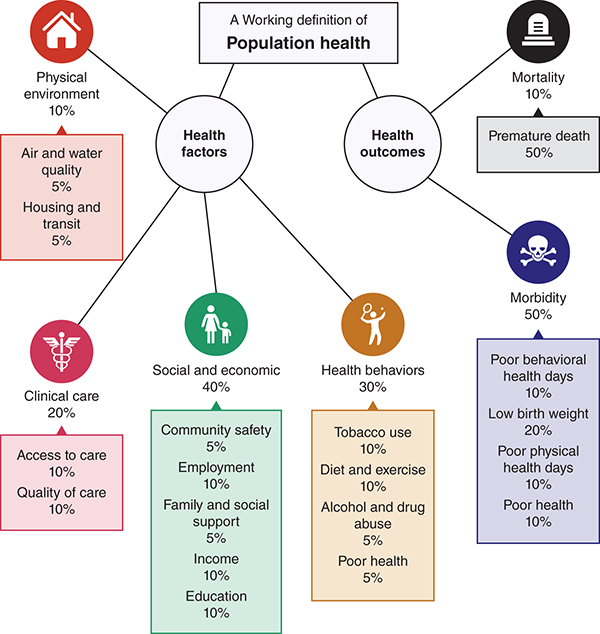
Long Description for Figure5.2
The percentage of each factor that contributes to health is as follows. Physical environment, 10 percent which includes air and water quality, 5 percent, and housing and transit, 5 percent. Clinical care 20 percent. It comprises access to care, 10 percent, and quality of care, 10 percent. Social and economic factors, 40 percent. It comprises community safety, 50 percent; employment, 5 percent; family and social support, 5 percent; income, 10 percent; education, 10 percent. Health behaviors, 30 percent. It includes tobacco use, 10 percent; diet and exercise, 10 percent; alcohol and drug abuse, 5 percent; poor health, 5 percent. Morbidity, 50 percent. It includes poor behavioral health days, 10 percent; low birth weight, 20 percent; poor physical health days 10 percent; poor health, 10 percent.
Research to understand the effects of health factors on health outcomes remains ongoing.
Although the responsibility for “performance” typically falls to public officials, public health agencies, or organizations that are not primarily deliverers of care, nurses have direct relationships with patients and communities and are obligated to advocate for the delivery of services.
Population Health Quality Measures
Content in this section was adapted from the U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality (2018).
Measures are applied to groups of persons identified by geographic location, organizational affiliation, or nonclinical characteristics to assess public health programs, community influences on health, or population-level health characteristics that may not be directly attributable to the care delivery system. These measures are supported by evidence demonstrating that they indicate the better or worse performance of population health activities (Table 5.1).
|
|
Definition |
Measures |
Example |
|---|---|---|---|
|
Population process |
A population process of care is a public health–related practice or service performed for, on behalf of, or by a population. |
|
The proportion of adults aged 65 years and older in a county who have received an influenza vaccination in the past year |
|
Population access |
Population access to care is the timely and appropriate receipt of a public health intervention by a population. |
|
The percentage of smokers in a county who reported that they were able to access a smoking-cessation program or, in the case of the nurse working to implement the syringe exchange program, the percentage of people accessing the syringe exchange to get clean injection supplies |
|
Population outcome |
A population outcome measures the health of a population resulting from a public health intervention. |
|
The proportion of children with elevated blood lead levels whose homes undergo lead remediation and whose blood lead levels are subsequently reduced to normal levels. Again, going back to the syringe exchange example, the proportion of people who inject drugs that have contracted hepatitis C since the inception of the syringe exchange program compared with the rate before the establishment of the syringe exchange |
|
Population structure |
Population structure of care is a feature of a public health program related to its capacity to provide high-quality public health services to a population. |
|
The number of licensed childcare facilities and slots in a county or how many needle exchange locations are available within the state |
|
Population experience |
Population experience is the report of the members of a population concerning observations of and participation in public health programs. |
|
The percentage of smokers in a county reporting that they have seen or heard public service announcements promoting a county health department–sponsored smoking-cessation program or the percentage of people who are aware that a syringe is available |
Related Population Health Measures
Content in this section was adapted from the U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality (2018).
Some population health measures will be applied to a group of people to assess public health programs, community influences on health, or population-level health characteristics that are not related to health care initiatives. These measures are not supported by evidence demonstrating a link to better or worse performance of population health activities (Table 5.2).
|
|
Definition |
Measures |
Example |
|---|---|---|---|
|
Population health state |
A population health state is the health status of a population. |
|
The prevalence rate of asthma in a county |
|
Population management |
Population management is a feature of a public health system that is relevant to the system’s administration, oversight, or staff. |
|
Whether a public health department uses competitive bidding to award contracts for social marketing campaigns |
|
Population use of services |
Population use of services is the provision of services to, on behalf of, or used by a population. |
|
The percentage of assisted-living facility beds that are occupied in a county |
|
Population cost |
Population costs of care are the monetary or resource units expended to deliver public health interventions to a population. Cost measures are computed from data in monetary or resource units. |
|
The average per beneficiary Medicaid expenditures in a county |
|
Population health knowledge |
Population health knowledge is the awareness and understanding of health-related information such as risk factors, prevention strategies, or treatment recommendations. |
The mean response score to a set of questions about HIV prevention |
|
|
Social determinants of health |
Social determinants of health are characteristics of a population related to social position or economic statuses, such as age, gender, or poverty status, that evidence has shown to be related to health states. |
The proportion of families living at or below the poverty level |
|
|
Environment |
Environment represents the conditions outside of the health care delivery system that may influence the health of a population. |
|
The number of days in the past year when the concentration of particulate air pollution in a community exceeds a defined threshold |
Population Efficiency Measures
Content in this section was adapted from the U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality (2018).
Measures that may be used to assess efficiency directly (e.g., by comparing a measure of quality with a measure of resource use) or indirectly (e.g., by measuring the frequency with which population health processes are implemented that have been demonstrated by evidence to be efficient; Table 5.3).
|
|
Definition |
Measures |
Example |
|---|---|---|---|
|
Population efficiency |
Efficiency of population health is the number of resources used to attain a specific level of quality on measures related to maintaining or improving the health of a population. |
|
Day case surgery rates, as a percentage of all surgery cases that could be treated in an outpatient setting in a county (based on evidence that day case surgery is equally or more effective and because day case surgery is presumably less costly) |
Population Health Strategies
The strategies for population health are as vast and varied as the populations they serve. Strategies for achieving better population health include:
- Understanding indicators and key metrics of health
- Engaging community stakeholders to act
- Assessing the needs and risks within the population or community
- Identifying evidence-based actions to improve health on a population scale
- Developing a shared vision, priorities, and plans amongst stakeholders
- Committing to shared resources and responsibilities
- Coordinating the implementation of health improvement programs
- Evaluating the effectiveness of processes and programs through community-based discussions and reevaluation of key health metrics
Effective population health strategy always begins with an evaluation of the population health data, using reputable sources, to determine the strengths and opportunities for a particular population. This begins with knowledge of where to find relevant sources of data and how to evaluate the data to understand the needs of the populations served. Sources of data typically include government organizations, nongovernmental organizations, research literature, academic centers of excellence, and others.
Benefits of a Population Health Approach
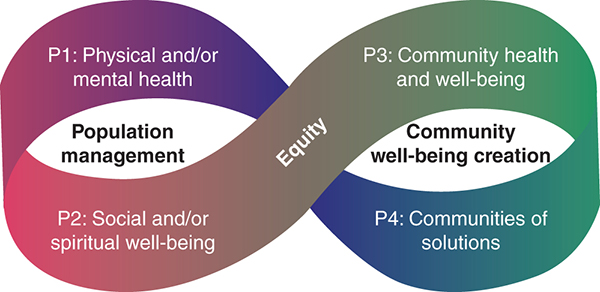
In 2014, Halfon and colleagues described a path for the evolution of the U.S. health care system from an Acute System (episodic, nonintegrated care) to a Coordinated, Seamless Health Care System (outcome-accountable care) to a Community-Integrated Health Care System (Halfon et al., 2014). These stages mirror the three buckets of prevention: traditional clinical prevention, innovative clinical prevention, and total population or community-wide prevention. The portfolios of population health framework (Figure 5.3), adapted from Institute for Healthcare Improvement (2022), builds on this important foundation with several modifications based on experience with supporting health care organizations in their efforts to improve population health.
Long Description for Figure [X]
Population management includes P 1, physical and or mental health, and P 2, social and or spiritual well-being. Community well-being creation includes P 3, community health and well-being, and P 4, communities of solutions. Equity connects to all aspects of the framework.
Two major domains of work emerged: efforts focused on the health and well-being of defined populations for whom health care organizations feel directly responsible, such as patients or employees (population management); and efforts focused on the health and well-being of communities (community well-being creation). These domains were further subdivided into four portfolios of population health on which improvement work is likely to focus (Table 5.4).
|
|
Portfolio 1: Physical and/or Mental Health |
Portfolio 2: Social and/or Spiritual Well-Being |
Portfolio 3: Community Health and Well-Being |
Portfolio 4: Communities of Solutions |
|---|---|---|---|---|
|
Type of population |
Defined |
Defined |
Place-based and defined |
Place-based and defined |
|
Focus of work |
Proactively address mental and/or physical health for the population for which an organization is directly responsible (e.g., patients, employees) |
Proactively address social and spiritual drivers for the population for which an organization is directly responsible (e.g., employees) |
Improvement of health, well-being, and equity focus on specific topics across a place-based or defined population) |
Whole community transformation with a focus on long-term structural changes needed for a thriving, equitable community |
|
Example activities |
Manage diabetes outcomes for a primary care panel; integrate mental health into primary care |
Screen for and address social determinants of health in a partnership with community social-service agencies; establish peer-to-peer supports |
Engage in a multisector partnership to address food insecurity in key neighborhoods |
Engage in a multisector partnership to create long-term structure, policy, and systems changes (e.g., preferred purchasing from minority-owned local businesses) |
Together, these four interconnected portfolios represent a comprehensive scope of population health–related improvements an organization may pursue. The four portfolios connect to and build on one another and are intended to represent a balanced portfolio of efforts that could be part of a health care organization’s overall population health improvement strategy. Consider each portfolio to be a force multiplier—that is, all four portfolios are necessary to achieve maximum impact. If one is missing or weak, the health care organization is likely missing an important part of its optimal population health strategy. In addition, the portfolios are not sequential, and any portfolio can be a starting point. While most health care organizations will likely have a predominance of activities in Portfolio 1, most organizations can identify some existing activity in all four portfolios. Health care organizations would be well served to develop an asset map to identify activities already underway in all four portfolios and then create a plan to develop a balanced portfolio of activities over time (Table 5.5).
|
|
Portfolio 1: Mental and/or Physical Health |
Portfolio 2: Social and/or Spiritual Well-Being |
Portfolio 3: Community Health and Well-Being |
Portfolio 4: Communities of Solution |
|---|---|---|---|---|
|
Roles to leverage |
|
Social service and community connector |
|
Community steward (in partnership with others), leveraging roles as
|
|
Relationships |
|
Partnerships are in place with agencies defined by the social service they provide (e.g., Alcoholics Anonymous, food bank, Union Mission). |
|
Partnerships are in place with agencies that focus beyond sectarian or defined areas (e.g., United Way, ministerial organizations, mayor’s office). |
|
Governance |
|
|
|
|
|
Financing models |
|
|
|
|
|
Policy |
|
|
|
|
|
Data |
|
|
|
|
|
Equity |
|
|
|
|
|
Partner with people with lived experience |
|
|
|
|
Finally, these portfolios are meant to be interconnected and synergistic. The more the activities across portfolios are balanced, the easier it may be to improve population health because each portfolio unlocks a set of relationships, capacities, and levers that a health care organization can use to create change. For meaningful transformation to occur within and across portfolios, factors such as partnering with those with lived experience and addressing equity, payment, and measurement are vital to success.
While describing four portfolios with concomitant activities is a great first step, we must still consider how we operationalize these efforts. The portfolios of population health table (Table 5.4) also outlines actions proposed by the Institute for Healthcare Improvement across a set of key levers deemed vital to accelerating improvements within and across portfolios. The actions are meant to build on each other, with actions described in Portfolio 1 also present in Portfolio 2. For visual clarity, however, these actions are not repeated across portfolios; only those actions that are unique to each portfolio are included in the table.
Examples of Population Health Programs and Initiatives
The Health Impact in 5 Years (HI-5) initiative highlights nonclinical, community-wide approaches that have evidence reporting positive health results within 5 years, and cost-effectiveness and/or cost savings over the lifetime of the population (CDC, 2022).
The health outcomes that HI-5 interventions can prevent or reduce are presented in the following list, which demonstrates the broad health impact that community-wide approaches can have:
- Anxiety and depression
- Asthma
- Blood pressure
- Bronchitis
- Cancer
- Cardiovascular disease
- Child abuse and neglect
- Cognitive development
- Infant mortality
- Liver cirrhosis
- Motor vehicle injuries
- Obesity
- Dental caries
- Pneumonia
- Sexually transmittable infections
- Sexual violence
- Teenage pregnancy
- Traumatic brain injury
- Type II diabetes
- Youth violence (CDC, 2022)
Many programs and initiatives focus on population health at the local, city, state, national, and global levels. Just as many programs exist that focus on specific disease states or metrics across multiple population levels. It is important to recognize that all these programs and initiatives are important drivers of change and that each contributes in small and large ways to improve population health.
The public health impact pyramid in Figure 5.4 highlights the different types of public health interventions, starting with those that have the greatest potential to affect health. The pyramid can be applied to any setting, but this scenario is applied to issues affecting children.
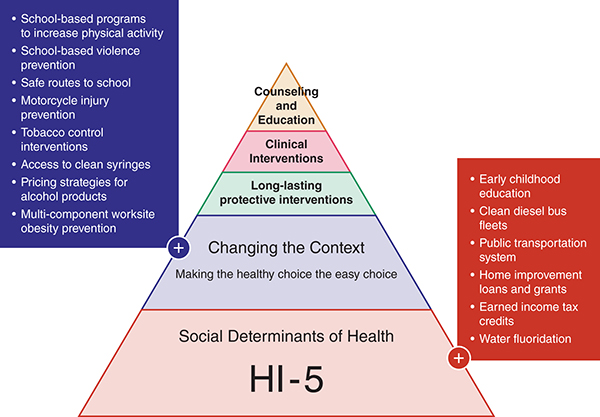
Long Description for Figure [X]
The layers of the pyramid represent the interventions as follows, from the base to the apex. Social determinants of health, HI-5, which includes early childhood education, clean diesel bus fleets, public transportation system, home improvement loans and grants, earned income tax credits, and water fluoridation. The next level is changing the context, or making the healthy choice the easy choice, which includes School-based programs to increase physical activity. School-based violence prevention. Safe routes to school. Motorcycle injury prevention. Tobacco control interventions. Access to clean syringes. Pricing strategies for alcohol products. Multi-component worksite obesity prevention. The top three levels are Long-standing protective interventions. Clinical interventions. Counseling and education.
The Nurse’s Role in Community and Population Health
Community health nurses aim to improve the health of community members. Community health nurses work in schools, churches, and government agencies. They focus on vulnerable populations, including socioeconomically disadvantaged families, people living in rural areas, immigrants, and individuals with disabilities. The relationship between community health nurses and their patients is one of shared responsibility for the patient’s health outcome (St. Catherine University, 2022).
Although the responsibilities of these nurses differ in each career path, all community health nurses promote healthy living, disease prevention, and access to health care. Community health nurses create programs that promote community health and collect data to identify community needs. The goal is to promote health and prevent disease and disability. Community health nurses’ knowledge and skills enable them to contribute significantly to public health. Their clinical knowledge and unique relationships with those they serve allow them to assist in designing and implementing policy-based programs to meet the needs of vulnerable populations. The combination of a clinical nursing background with knowledge from the public health and social sciences provides a sound basis for public health leadership positions (Association of Public Health Nurses, 2022).
Examples of public health nursing activities include the following:
- Evaluating health trends and risk factors of population groups and helping to determine priorities for targeted interventions
- Working with communities or specific population groups within the community to develop public policy and targeted health promotion and disease prevention activities
- Participating in assessing and evaluating health care services to ensure that people are informed of available programs and services and assisted in the utilization of those services
- Providing essential input to interdisciplinary programs that monitor, anticipate, and respond to public health problems in population groups
- Providing health education, care management, and primary care to individuals and families who are members of vulnerable populations and high-risk groups
Public health nurses also provide a critical linkage between epidemiological data and clinical understanding of health and illness as it is experienced in people’s lives. This understanding is translated into action for the public good (Association of Public Health Nurses, 2022). It is important to recognize just how essential community health nurses are to bridge the gap between policy and patient-centered care and to ensure that populations have access to the programs they need to improve health outcomes.
Practice Application
➔ Setting the Scene
As a part of their support for community health, nurses can be involved in initiatives to reduce community tobacco use, increase the use of park spaces for exercise, or reduce childhood asthma attacks in school for a particular population. A nurse may undertake these efforts by doing any of the following:
- Evaluating the data on the topic for a chosen population using public health data sets and metrics. A full data evaluation may not be required, but the main issues (outcomes) surrounding the topic—such as mortality rates, incidence, prevalence, and years of life lost—need to be considered to gain a good understanding of the impact and burden of this disease or condition within the community.
- Reaching out to community partners such as a local organization, school, religious center, local government office, or health center to identify potential opportunities for collaboration.
- They may already have an existing initiative to become involved with.
- If not, they may need incentives for the partnership. What benefits would the partnership bring to the organization? Develop this as a “win-win.”
➔ Think About It
Use the Healthy People 2030 website to select a health issue in your community, such as tobacco use, lack of exercise space, or asthma triggers in K–12 schools. Imagine you are a nurse working to build an initiative to combat this issue.
- What data will be helpful in evaluating this issue? Where can you locate the needed data?
- How helpful was Healthy People 2030 in gathering needed information? What was missing from this site?
- What are the stakeholders for this issue?
- What work on this issue, if any, is already occurring in each of the four portfolios of population health?
- Which community organizations will be helpful partners for your initiative?
- Do these organizations already have aligned initiatives?
- What incentives may be needed to get the organizations to partner?
- What other information is needed to organize your initiative?
Additional Resources
CDC – 6 | 8 Initiative: Accelerating Evidence into Action
CDC – Health Impact in 5 Years
CDC – Preventing Excessive Alcohol Use
CDC – Youth Risk Behavior Survey Report
St. Catherine University – What Is a Community Health Nurse? (Career Overviews)
References
Agency for Healthcare Research and Quality. (2018). NQMC measure domain definitions. www.ahrq.gov/gam/summaries/domain-definitions/index.html
Arnetz, B. B., Goetz, C. M., Arnetz, J. E., Sudan, S., vanSchagen, J., Piersma, K., & Reyelts, F. (2020). Enhancing healthcare efficiency to achieve the Quadruple Aim: An exploratory study. BMC Research Notes, 13, 362. https://doi.org/10.1186/s13104-020-05199-8
Association of Public Health Nurses. (2022). What is a PHN? www.phnurse.org/what-is-a-phn-
Berwick, D. M., Nolan, T. W., & Whittington, J. (2008). The Triple Aim: Care, health, and cost. Health Affairs (Project Hope), 27(3), 759–769. https://doi.org/10.1377/hlthaff.27.3.759
Boehringer Ingelheim Pharmaceuticals. (2021). Quadruple Aim. Strategies for Quality Care. www.strategiesforqualitycare.com/quadruple-aim
Centers for Disease Control and Prevention. (2020, October 6). What is population health? Population Health Training in Place Program (PH-TIPP). https://archive.cdc.gov/#/details?url=https://www.cdc.gov/pophealthtraining/whatis.html
Centers for Disease Control and Prevention. (2022). Health impact in 5 years. https://www.cdc.gov/policy/hi5/index.html
Halfon, N., Long, P., Chang, D. I., Hester, J., Inkelas, M., & Rodgers, A. (2014). Applying a 3.0 transformation framework to guide large-scale health system reform. Health Affairs (Project Hope), 33(11), 2003–2011. https://doi.org/10.1377/hlthaff.2014.0485
Institute for Healthcare Improvement. (2022). Resources. https://www.ihi.org/resources
Institute of Medicine (US) Committee for the Study of the Future of Public Health. (1988). Summary and recommendations. In The future of public health. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK218215/
Nundy, S., Cooper, L. A., & Mate, K. S. (2022). The Quintuple Aim for health care improvement: A new imperative to advance health equity. JAMA, 327(6), 521–522. https://doi.org/10.1001/jama.2021.25181
Saha, S., Loehrer, S., Cleary-Fisherman, M., Johnson, K., Chenard, R., Gunderson, G., Goldberg, R., Little, J., Resnick, J., Cutts, T., & Barnett, K. (2017). Pathways to population health: An invitation to health care change agents. https://www.ihi.org/sites/default/files/2023-09/Pathways-to-Population-Health_Framework.pdf
St. Catherine University. (2022). What is a community health nurse? www.stkate.edu/academics/healthcare-degrees/community-health-nurse
The George Washington University. (2015, April 27). What is population health? Milken Institute of Public Health. https://onlinepublichealth.gwu.edu/resources/what-is-population-health/
Virginia Hospital & Healthcare Association. (2015, July 17). Defining population health. Data Analytics.
