
Chapter Three: Social Determinants of Health and Vulnerable Populations
Overview
This chapter presents foundational information on social determinants of health (SDOH) and vulnerable populations. These determinants are critical to improving health, advancing health equity, and reducing health disparity. Research indicates that health outcomes are a result of multiple variables, including underlying genetics, health behaviors, social and environmental factors, and health care. Vulnerable populations are groups of people and communities at a higher risk for poor health as a result of the barriers they experience, including social, economic, political, and environmental resources, as well as limitations caused by illness or disability (National Collaborating Centre for Determinants of Health, 2022).
Learning Objectives
- Identify the SDOH and how they influence the health status of individuals, communities, and populations
- Recognize the impact of health disparities and SDOH on care outcomes
- Recognize how geospatial determinants of health can make the connection between “place” and health
- Connect SDOH principles with vulnerable populations
Key Terms
- social determinants of health
- geospatial determinants of health
- health behaviors
- vulnerable populations
Content in this chapter was adapted from Healthy People 2030.
Introduction
Public and community health nurses are in an ideal position to integrate a holistic understanding of SDOH and recognize the unique health risks to vulnerable populations. Public health nurses assess, identify, and intervene to improve the health and health outcomes of individuals, families, and populations.
Social Determinants of Health
A significant portion of health can be attributed to social and environmental factors, separate from medical care or a person’s individual lifestyle choices. In fact, medical care itself may account for only 10%–20% of an individual’s health outcomes, while approximately 80%-90% of the factors that influence health can be linked with SDOH (Magnan, 2017). Social determinants of health comprise the conditions where people are born, work, live, worship, age, and play that affect an individual’s health, functioning, quality of life outcomes, and risks (Magnan, 2017; U.S. Office of Disease Prevention and Health Promotion [ODPHP], 2022e; Kaiser Family Foundation, 2018).
Social determinants of health can be broadly grouped into five categories: economic stability, educational access and quality, neighborhood and built environment, health access and quality, and social and community context (ODPHP, 2022k). Nurses should recognize that a person’s health consists of a few different factors, and only one of those factors is the individual’s health behaviors. As Figure 3.1 demonstrates, socioeconomic factors and physical environment, both SDOH components, are major factors in a person’s overall health.
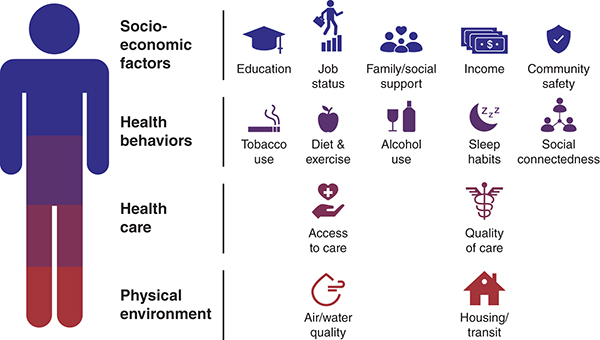
Long Description for Figure 3.1
Socio-economic factors include education, job status, family or social support, income and community safety. Health behaviors include tobacco use diet and exercise, alcohol use, sleep habits, and social connectedness. Healthcare includes access to care and quality of care. The physical environment includes air and water quality and housing transit.
Social determinants contribute to wide health disparities and inequities. For example, people who do not have access to grocery stores with healthy foods are less likely to have good nutrition, raising their risks for health conditions such as heart disease, diabetes, and obesity and lowering life expectancy relative to people who do have access to healthy foods. Nurses then must understand the conditions in which people live, work, play, and pray to understand their patients’ barriers to and facilitators of good health. Nurses in the community must realize the impact that social determinants can have on patients’ health outcomes and then address those determinants through the alleviation of barriers.
Social determinants can also influence specific health behaviors, such as diet and exercise, which can further drive health outcomes. For example, in terms of education, families with parents who have not completed high school are more likely to live in a neighborhood that poses barriers to health, such as lack of safety, exposed garbage, and substandard housing. They are also less likely to have access to healthy and safe community environments, including sidewalks, parks or playgrounds, recreation centers, or a library. Further, the stress that results from these less than optimal environments is shown to negatively affect health across the lifespan, and these environmental factors may have multigenerational impacts. Addressing SDOH is not only critical to improving the overall health of individuals, communities, and society as a whole. It is vital to reduce health disparities that are often rooted in social and economic disadvantages.
Examples of SDOH include:
- Safe housing, transportation, and neighborhoods
- Racism, discrimination, and violence
- Education, job opportunities, and income
- Access to nutritious foods and physical activity
- Polluted air and water
- Language and literacy skills (ODPHP, 2022k)
In this chapter, we provide a few selected examples of priorities within each SDOH category, discuss these factors’ impact on achieving good health, and provide context for actions that can be taken to help address SDOH.
Economic Stability
Economic security is having stable, sufficient income to meet your basic needs, while economic insecurity is living in a household with incomes below 200% of the federal poverty level. Today one out of every three people in the United States is economically insecure. Economic security for households and residents is essential for the health and well-being of families, neighborhoods, and local and national economies. In 2022, several tax policies enacted by the American Rescue Plan Act (ARPA) in 2021 lapsed, including expanding the earned income tax credit for filers without children and full refundability of the child tax credit and child and dependent care credit. The contraction in federal tax programs led to a substantial decline in real posttax incomes. The U.S. Census Bureau’s real median posttax household income in 2022 was 8.8% lower than in 2021.
Economic stability can be described as the ability to access resources essential to one’s life and well-being. The federal poverty level is the standard proxy measure to indicate whether individuals or families are poor or unable to meet their basic economic needs. In 2022, the U.S. Census Bureau reported that 11.5% of the population, or 37.9 million people, lived in poverty. Healthy People 2030 has identified unemployment or underemployment, food insecurity, housing instability, and poverty as factors directly influencing economic stability (ODPHP, 2022a).
Food Insecurity
A household experiences food insecurity when facing recurrent barriers to accessing enough food to live a healthy and active life (Feeding America, 2022). In 2020, there were 38.3 million people living with some level of food insecurity, and 584,000 children were living in households with very low food security (United States Department of Agriculture [USDA], Economic Research Service, 2022). The USDA divides food insecurity into two categories:
- Low food security: “Reports of reduced quality, variety, or desirability of diet. Little or no indication of reduced food intake.”
- Very low food security: “Reports of multiple indications of disrupted eating patterns and reduced food intake.”
The type of household a person lives in greatly affects the prevalence of food insecurity. Households with children have higher rates of food insecurity, as also do households that are headed by a single woman, Black non-Hispanic households, and Hispanic households. Some urban and rural neighborhoods have very few full-service supermarkets for residents to frequent. Often, urban neighborhoods have small corner stores with processed food options and limited options for fresh, healthy foods. Additionally, the cost markup for these types of markets tends to be higher than for other grocery stores, effectively limiting the amount of food that local residents can buy. Lack of public transportation also affects a family’s ability to obtain food, particularly for families living in rural areas without access to personal vehicles and without public bus routes.
Food insecurity is linked to negative health outcomes in children and adults, and being hungry or malnourished can lead to decreases in school performance. Helping to reduce hunger by addressing unemployment and providing access to nutrition assistance programs can help families achieve better overall health. Food assistance programs—such as the National School Lunch Program (NSLP), the Women, Infants, and Children (WIC) program, and the Supplemental Nutrition Assistance Program (SNAP)—address barriers to accessing healthy food. Nurses can help by making sure the families they care for know about these programs and help families to get signed up for assistance (ODPHP, 2022d).
Housing
There are complex reasons for housing instability that can include many variables, among them having trouble paying rent, overcrowding, moving frequently, or spending the bulk of household income on housing. If more than 30% of a household’s income is spent on housing, that household is considered to be cost-burdened; if more than 50%, then the householders are considered to be severely cost-burdened (Bailey et al., 2016). A limited rental market with few affordable vacancies may force people with the lowest incomes to rent substandard housing or force individuals to share housing, resulting in overcrowding. When housing costs are more than a household can reasonably afford, it can lead to foreclosures, which cause a loss of money and possessions and can damage the social fabric of neighborhoods.
Multiple forced moves as a result of housing instability have been associated with negative health outcomes in children. For individuals, housing instability can lead to a greater incidence of poor health outcomes, from mental health issues to heightened stress levels, to relationship injury, and to a greater likelihood of infectious disease transmission (ODPHP, 2022f).
Housing deprivation at its most severe leads to people without homes and with health issues: a study of newly unhoused people “in the New York City shelter system found that 6% had diabetes, 17% had hypertension, 17% had asthma, 35% had major depression, and 53% had a substance use disorder—indicating that chronic disease is more common among people who are newly homeless than among the general population” (Schanzer et al., 2007).
Educational Access and High School Graduation Rates
People with higher levels of education are more likely to be healthier and live longer than those with low levels of education. Providing high-quality educational opportunities for children and adolescents, and helping them do well in school, can ultimately also help them achieve better health. A child who struggles with math and reading could potentially be experiencing a learning disability, living in a low-income situation, or facing social discrimination. These children are less likely to graduate from high school, which limits their ability to secure safe, well-paying jobs. Barriers such as poverty can lead to greater health problems, such as heart disease, depression, and diabetes. Some children live in areas where the schools are performing poorly, school resources are limited, and attaining the same level of education as someone in a higher-performing school is outside their control. Additionally, if these children live in poverty, they are more likely to be affected by delayed brain development, making it even harder for them to do well in school. Targeted interventions to support educational access and quality, such as taking preventive mental health measures and improving high school graduation rates, can help children have better health in the long term (ODPHP, 2022b).
Higher levels of education are also linked to a lower risk of early death later in life. Many high school students do not graduate, and graduation rates are lower in some racial/ethnic groups. Students from economically disadvantaged families often have less access to resources, and they tend to live in communities with underperforming schools. These factors may contribute to lower academic achievement and higher dropout rates as compared with students from economically advantaged families. In 2015, the number of young people aged 16 to 24 who did not complete high school or were not enrolled in high school was 4.1 times higher in low-income families compared with high-income families (ODPHP, 2022g). High school graduation is important for many reasons, but primarily because the skills learned help support the attainment of a safe, high-paying job or successful college attendance. The ability to secure stable employment and income helps support conditions where people can achieve better health.
Programs that offer vocational training, alternative schools, social-emotional skills training, and/or counseling can help more students graduate from high school. Research shows that high school graduates have better employment prospects and lifelong earning potential than do nongraduates. For every year of high school a student completes, their lifetime wealth increases by 15%. Overall, high school graduation has the potential to improve population health (ODPHP, 2022g).
Preventive Mental Health in Schools
Anxiety and depression are common among children—even more so in the wake of the recent COVID-19 pandemic, when children were suddenly restricted from engaging in their normal social outlets with teachers and friends. For many children, the lengthy distance-learning periods while schools were physically closed meant that students spent a significant amount of time looking at computer screens without the recess, lunch, physical education, and social breaks that are beneficial to mental health. Children who routinely experience forms of social discrimination—like bullying—are more likely to struggle with math and reading and less likely to graduate from high school or go to college (Community Preventive Services Task Force, 2019). Increasing the proportion of children who receive preventive mental health services in school is a high-priority public health issue. Targeted school-based therapy programs are intended to reduce depression and anxiety in school-aged children and adolescents at increased risk for these conditions. Trained school staff or outside mental health professionals deliver these interventions in individual or group settings that helps students build strategies for problem-solving, emotional regulation, and helpful behavior patterns.
Neighborhood and Built Environment
In the United States, many people live in neighborhoods with high rates of violence, unsafe air or water, and other health risks, a situation that greatly affects their health and well-being. People with low incomes and members of racial/ethnic minorities are more likely to live in places with these risks. Likewise, individuals may be exposed to conditions at work that can harm their health. There are government interventions and policy changes that can reduce health and safety risks and promote health, such as providing opportunities for people to walk and bike in their communities by adding sidewalks and bike lanes. These types of interventions can increase safety and help improve health for communities (ODPHP, 2022i).
Geospatial Determinants of Health
The places a life is lived—from home to workplace, schools to parks, and town centers to places of worship—all affect the health of individuals and their communities, directly influencing how people experience disease and well-being. Geospatial science, geographic information systems, and cartographic visualization provide important methods and tools that public health scientists use to analyze the critical relationship between health and the places lives are lived.
The Geospatial Research, Analysis, and Services Program, commonly referred to as GRASP, is developing a framework for the specific geospatial determinants of health to (1) define the geospatial drives of health with an emphasis on factors that vary by place; (2) serve as a catalyst to define, promote, and advance the use of place in research and practice across the public health community; and (3) shape the public health curriculum of schools across the United States to advance geospatial analysis, statistics, and technology in the study of public health (Agency for Toxic Substances and Disease Registry, n.d.).
Environmental Conditions
The quality and state of the environment, or environmental conditions, are part of daily life that can affect health and can vary widely among populations and geographic locations. Although many of the conditions people experience in the environment are naturally occurring, the quality of an environment can be affected by historical, economic, and sociopolitical factors detailed in the literature summarized in Healthy People 2030: Environmental Conditions as a social determinant of health (ODPHP, 2022c).
Populations that may be more susceptible to poor environmental conditions and their associated health disparities include communities of color, persons with low incomes, persons who are unhoused, older adults, pregnant women, and children. The rising temperatures and shifting weather patterns around the globe, a result of climate change, are expected to worsen public health challenges, particularly for disadvantaged communities (ODPHP, 2022c). Policies and programs that can have an impact on environmental conditions have been effective in reducing the harmful effects of pollutants. For example, federal laws, such as the Clean Air Act and Safe Drinking Water Act, regulating air and water quality, have successfully reduced the harmful health effects of pollutants (Weinmeyer et al., 2017; Nethery et al., 2021). As environmental conditions continue to evolve, additional innovative and sustainable interventions are needed to address the effects of environmental conditions on health outcomes and disparities.
Water Quality
As an essential part of human life, water quality is critical to the environment and to health and well-being. The U.S. water supply is generally safe, but water can be contaminated in a variety of ways, such as through certain agricultural practices, sewage leaks, or naturally occurring harmful substances. Water may also be contaminated with pathogens, which cause waterborne diseases, or with chemicals, which cause other negative health issues (Centers for Disease Control and Prevention [CDC], 2022b). There are approximately 7.15 million cases of waterborne illnesses from pathogens alone in the United States each year (CDC, 2020).
The Safe Drinking Water Act was established in 1974 to regulate drinking water by setting national standards for over 90 contaminants (U.S. Environmental Protection Agency, 2015). Water quality may still be affected by several natural, built, and sociopolitical factors, which can lead to health disparities (Balazs & Ray, 2014; Schaider et al., 2019). Many factors can influence the quality of a community’s water, from the number of institutions or individuals dedicated to managing a water system to the size of a water source, to city planning decisions (ODPHP, 2022c). Communities with lower incomes and communities of color have been found to have a higher risk of exposure to water quality health violations and water contaminants, such as arsenic and nitrates. Furthermore, the Safe Drinking Water Act does not regulate small, private wells, often putting rural residents, who are more likely to use private well water, at risk, particularly for high levels of nitrates (ODPHP, 2022c). High levels of nitrate or arsenic exposure can cause nausea, vomiting, cardiovascular issues, and death (Agency for Toxic Substances and Disease Registry, 2015, 2017).
Air Quality
Like water, air is a vital condition for life and health. However, air pollution is associated with an estimated 100,000 to 200,000 deaths annually in the United States (Tessum et al., 2019). Particles commonly emitted into the air by motor vehicles, industrial facilities, and fires—such air pollutants as carbon monoxide, ozone, nitrogen and dust, smoke, and drops of liquid—affect air quality (ODPHP, 2022c). Poor air quality is linked to many health problems, including lung cancer and heart disease (Turner et al., 2011). There are also naturally occurring particles, including pollen, that can cause allergic reactions and respiratory concerns that substantially affect community health (Saha et al., 2021).
Urban areas often have more pollution sources, resulting in worse air quality when compared with rural areas. Additionally, as a result of historical, sociopolitical, and discriminatory factors, communities of color encounter air pollution more often than predominantly White communities do. For example, neighborhoods of color are more likely to be located near pollution sources, such as factories and industrial facilities, as a result not only of discriminatory city planning but also of the residents’ limited sociopolitical influence (Mikati et al., 2018; Woo et al., 2019).
Climate Change
The impacts of human-induced climate change are rapidly increasing and pose a real and significant threat to the health of the American people. As the U.S. Global Change Research Program (2016) notes, “Rising greenhouse gas concentrations result in increases in temperature, changes in precipitation, increases in the frequency and intensity of some extreme weather events, and rising sea levels.” Climate change endangers individuals and population health by affecting food and water sources, the air that people breathe, the weather that people experience, and people’s interactions with both built and natural environments. The risks to human health continue to expand as the climate continues to change, with current and future climate changes exposing more people in more places to public health threats.
Already in the United States there are observable climate-related increases in people’s exposure to elevated temperatures; more frequent, severe, or longer-lasting extreme events; degraded air quality; diseases transmitted through food, water, and disease vectors (such as ticks and mosquitoes); and stresses to individuals mental health and well-being. These threats are expected to worsen with continued climate change, and while all Americans are at risk, some populations are disproportionately vulnerable, including “those with low income, some communities of color, immigrant groups (including those with limited English proficiency), Indigenous peoples, children, and pregnant women, older adults, vulnerable occupational groups, persons with disabilities, and persons with preexisting or chronic medical conditions” (U.S. Global Change Research Program, 2016).
For more on climate change, visit The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment (globalchange.gov).
Noise Pollution
Increased exposure to human-made noise, such as traffic, is called noise pollution. Noise pollution has been associated with hearing loss, among other health issues, with some studies finding that noise pollution disproportionately affects communities of color and communities with low incomes (Casey et al., 2017).
Hazardous Waste Threats
There are health concerns for communities living near hazardous waste sites, such as industrial facilities, municipal waste sites, or incinerators; these health concerns include adverse pregnancy outcomes, childhood cancer, and other diseases (Brender et al., 2011; Orr et al., 2002). For example, one study found that adults living in the United States near a coal-burning power plant were more likely to report respiratory, gum, and skin conditions than were adults not living near a power plant (Zierold et al., 2020).
Health Care Access and Quality
Many people in the United States are unable to obtain the health care services they need, either because they have limited access to care or because the quality of care they are receiving is low. Around 10% of people in the United States do not have health insurance (Berchick et al., n.d.), which makes them less likely to have a primary care provider and to afford the health care services and medications they need. For persons who are uninsured or underinsured, the ability to obtain preventive care services and treatment for chronic illness depends on their finances. Increasing insurance coverage for people in the United States means they can get the necessary health care services. Sometimes people do not get recommended health care services, like cancer screenings, because they do not have a primary care provider. Other times, it is because they live too far away from a health care provider who accepts their type of insurance, offers sliding scale services, or specializes in the care they need.
Differences in quality of care contribute to poor health outcomes just as much as limited access to care does (ODPHP, 2022e). In 2002, the Institute of Medicine reported that racial and ethnic minorities tend to receive a lower quality of care. This is true even when issues such as lack of insurance or limited access to health care are controlled (Brummer et al., 2016). Higher rates of heart disease, cancer, diabetes, obesity, depression, infant mortality, and maternal morbidity are just a few examples of health disparities partially resulting from low-quality care. Interventions to increase access to health care professionals and improve care quality can help more people get and stay healthy (ODPHP, 2022e).
Family Planning
Almost half of the pregnancies in the United States are unintended, and unintended pregnancy is linked to negative outcomes for both individuals who are pregnant and infants (CDC, 2021b). With the overturning of Roe v. Wade and the changing legislation surrounding access to abortion services, a community health focus on family planning is as important as ever. Abortion restrictions disproportionately affect people of color and those with low incomes. According to the CDC, Black women are five times more likely to have an abortion than White women, and Latinx women are two times as likely as White women (CDC, 2022a). Of all people who have abortions, 75% are low income or poor. Reproductive health restrictions also affect women’s earning potential. Studies indicate that an absence of abortion restrictions would translate to between 1.5% and 2.5% increases in the labor force for Black, Hispanic, and Pacific Islander women. This translates to an estimated $13.4 million in increased earnings at the state level for Black women alone (Winny et al., 2021).
Adolescents are at especially high risk for unintended pregnancy. Close to 200,000 babies are born to teen mothers every year in the United States, and this is a reduction in rates from previous years. Abortion restrictions most negatively affect individuals who can become pregnant and teens who already have other negative SDOH working against them.
Data confirm significantly higher pregnancy-related mortality ratios among Black and American Indian/Alaskan Native women compared with other groups. These gaps did not change over time (Figure 3.2).
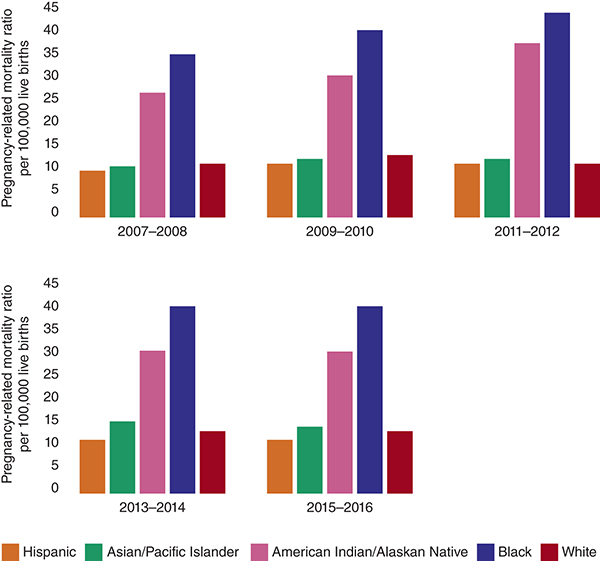
Long Description for Figure 3.2
The vertical axis measures the pregnancy-related mortality ratio per 100,000 live births with values ranging from 0 to 45. 2007 to 2008: Hispanic, 10. Asian or Pacific Islander: 10. American Indian or Alaskan Native: 25. Black: 35. White, 10. 2009 to 2010: Hispanic, 10. Asian or Pacific Islander: 11. American Indian or Alaskan Native: 30. Black: 40. White, 13. 2011 to 2012: Hispanic, 10. Asian or Pacific Islander: 10. American Indian or Alaskan Native: 35. Black: 45. White, 10. 2013 to 2014: Hispanic, 10. Asian or Pacific Islander: 15. American Indian or Alaskan Native: 30. Black: 40. White, 13. 2015 to 2016: Hispanic, 10. Asian or Pacific Islander: 12. American Indian or Alaskan Native: 30. Black: 40. White, 12. All data are approximate.
Sexually active women who do not want to get pregnant need access to birth control, but many individuals cannot afford effective birth control methods. Interventions such as publicly funded birth control are critical in reducing unintended pregnancies. Linking adolescents to youth-friendly health care services can help prevent pregnancy as well as sexually transmitted infections in this age group. Increasing the use of birth control and family planning services may help, in some situations, to reduce the negative health consequences associated with unintended pregnancy. Unintended pregnancy is linked to outcomes like preterm birth and postpartum depression.
Specific interventions suggested by the CDC include examining the need for contraceptive services among women of reproductive age, developing evidence-based strategies to reduce unmet needs for quality family planning services, and building capacity for health care providers, states, communities, and partners to improve quality family planning services.
Social and Community Context
Relationships and interactions with family, friends, coworkers, and community members can significantly affect an individual’s health and well-being. Ensuring that people get the social support they need in the places where they live, work, learn, and play is important.
Unsafe neighborhoods, discrimination, and trouble affording the things an individual or family needs are often challenges outside an individual’s control and can have a negative impact on health and safety throughout an individual’s life. Some individuals do not receive the support they need from loved ones or from others; these individuals may be children whose parents are in jail or bullied adolescents. Positive relationships at home, work, and within the community can help reduce these negative impacts, And interventions to help people access the social and community support they need are critical for improving health and well-being.
Families That Read Together
In 2019, only 55% of children aged 5 and under had a parent or caregiver who read to them at home (ODPHP, 2022h). Studies show that reading to young children improves their language and literacy skills and is linked to better behavior and health. Reading and health go hand in hand throughout life. Children’s behavior improves when they are confident in their reading abilities in school. Readers are encouraged to do their best and receive positive feedback, which sets the foundation for their self-esteem. However, children who struggle with reading might be withdrawn in class and lack self-esteem, and consequently when called on to read they may act out to avoid calling attention to their reading problems. Children might also feel headaches, stomach aches, and fatigue, the physical effects of the anxiety and embarrassment associated with reading struggles.
A further complication is that adults with low literacy skills have 3.5 times the health care costs that literate adults have (Nemours Foundation, 2022). So, it is important to consider methods to help children increase language and reading readiness. These methods include reading with a caregiver for at least 10 minutes a day, having a variety of books accessible in the home, and limiting screen time. Parents and children can share routines, build stronger relationships, and have regular positive interactions through reading out loud. Early intervention programs and national initiatives can help raise awareness about the importance of reading to children, but early and consistent reading in individual social circles is the first step toward healthier outcomes.
Bullying
Bullying of youth is a form of violence and is considered an adverse childhood event. It is a serious problem with serious morbidity and mortality consequences in our communities. Bullying can result in physical injury, social and emotional distress, self-harm, and even death. Youth who bully others are at increased risk for substance misuse, academic problems, and experiencing violence later in adolescence and adulthood. Data from the Youth Risk Behavior Surveillance Survey indicated that almost 20% of students were bullied on school grounds, and 15% had been bullied online (Kann, 2018).
Sexual minority students are at an increased risk of being bullied, especially in conservative or religious districts, where hateful behaviors toward them may often go unchecked by teachers and administrators. Nearly one third of sexual minority (LGBTQIA+) students in grades 9–12 reported that they experienced bullying at school (ODPHP, 2017). High school students who identify as lesbian, gay, or bisexual are almost twice as likely to be bullied as those who identify as heterosexual. Students who are bullied are more likely to have depression, anxiety, and sleep problems—and to drop out of school. As a result of the constant harassment, bullied individuals suffer academically, physically, and emotionally.
School-based programs to reduce violence can help prevent bullying of LGBTQIA+ students. Current bullying prevention efforts include anti-bullying laws and policies at the state, local, and school district levels. Newer efforts toward anti-bullying policies seek to enumerate the specific characteristics of children who are likely to be bullied, among them LGBTQIA+ students, in an effort to create targeted education and campaigns for bullying prevention. Enumerated anti-bullying policies not only define and denounce bullying but also list examples of characteristics that might be the basis of bullying, such as actual (e.g., a student is openly gay) or perceived (e.g., others think that a student is gay) sexual orientation.
Figure 3.3 suggests several protective risk factors and actions nurses can take to help prevent bullying in their communities (CDC, 2021a).
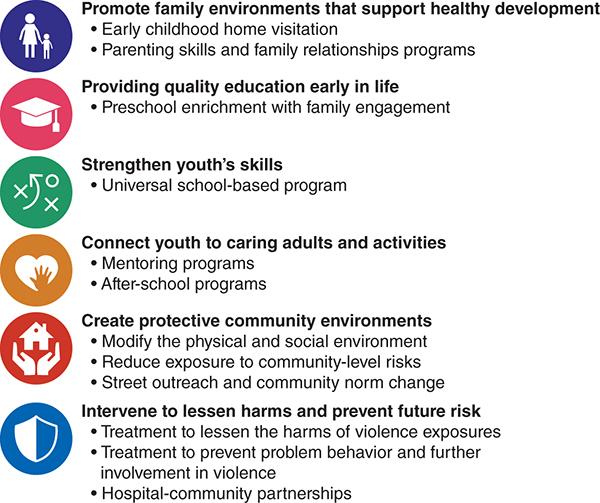
Long Description for Figure 3.3
Promote family environments that support healthy development includes early childhood home visitation and parenting skills and family relationships programs. Providing quality education early in life includes preschool enrichment with family engagement. Strengthen youth’s skills. It includes universal school-based program. Connect youth to caring adults and activities includes mentoring programs and after-school programs. Create protective community environments includes modifying the physical and social environment, reducing exposure to community-level risks and street outreach and community norm change. Intervene to lessen harms and prevent future risk includes treatment to lessen the harms of violence exposures, treatment to prevent problem behavior and further involvement in violence and hospital-community partnerships.
Vulnerable Populations
Many populations are considered vulnerable in the United States, including racial/ethnic groups, the economically disadvantaged, those with chronic health conditions, the LGBTQIA+ community, veterans, the HIV community, refugees and immigrants, the incarcerated, and differently abled populations, among others. Additionally, vulnerable populations may include rural residents, who often face barriers to accessing health care (AJMC, 2006; Joszt, 2018). Significant disparities exist in health care for these vulnerable groups, and health and health care problems can intersect with social factors, such as housing, poverty, and education. The percentage of the population that falls into vulnerable categories is significant. In just one example, Figure 3.4 illustrates the percentage of the adult population in the United States with specific functional disabilities.
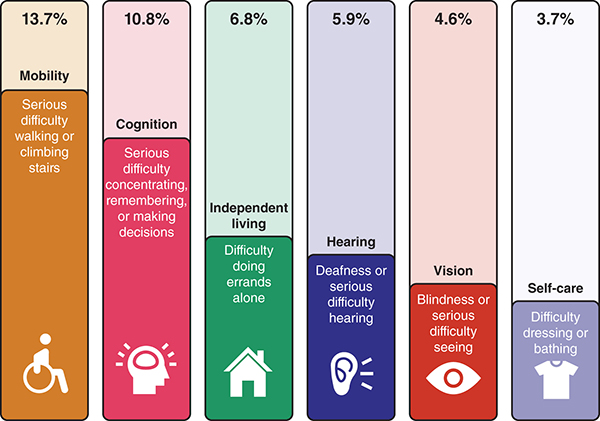
Long Description for Figure 3.4
13.7 percent have mobility issues such as serious difficulty walking or climbing stairs. 10.8 percent have cognition issues such as serious difficulty concentrating, remembering or making decisions. 6.8 percent have issues related to independent living such as difficulty doing errands alone. 5.9 percent have hearing issues such as deafness or serious difficulty hearing. 4.6 percent have vision problems such as blindness or serious difficulty seeing. 3.7 percent have self-care issues such as difficulty dressing or bathing.
Health Domains of Vulnerable Populations
Health domains of vulnerable populations may be divided into several categories, including the physical, psychological, and social. Examples of physical needs could include high-risk mothers and infants and those with chronic medical conditions such as diabetes or heart disease. Among older individuals, there is often more than one chronic condition, with much of this population having two or more chronic illnesses (AJMC, 2006).
Within the psychological domain, chronic mental conditions may include bipolar disorder, attention-deficit/hyperactivity disorder, substance abuse, and schizophrenia. Within the social realm, vulnerable populations can include those living in abusive families, people without homes, immigrants, and refugees (AJMC, 2006).
The health needs of these populations can be debilitating and are often compounded when an individual has issues in multiple domains.
The Need to Focus on Vulnerable Populations
The needs of medically vulnerable populations are serious and can be life-threatening, often requiring extensive nonmedical as well as medical services. Additionally, chronic illnesses are much more prevalent among economically disadvantaged populations. For example, patients with chronic illnesses who have less than a high school education are three times more likely to report being in poor health than those with the same illness who have an advanced degree (Robert Wood Johnson Foundation, 2002; AJMC, 2006).
Multiple risk factors within vulnerable populations intensify problems to make it more likely that health needs will not be adequately addressed. “Low income, no health insurance coverage, and lacking a regular source of care are closely related risk factors that build upon each other to influence the likelihood of having an unmet health need due to cost” (AJMC, 2006).
Vulnerable populations, defined as those at greater risk for poor health status and health care access, also may experience significant disparities in life expectancy, in access to and use of health care services, and in morbidity and mortality. Health needs for these populations are complex and intersect with the social and economic conditions they experience. Interventions are critical not only at the individual level but also at the local, state, and federal levels—where policy and legislation can mitigate the needs of vulnerable populations—because the strain on individuals, their community, and existing health care systems is great (AJMC, 2006).
Figure 3.5 illustrates several examples of vulnerable populations and specific mitigation and intervention measures that nurses working in community health settings may take.
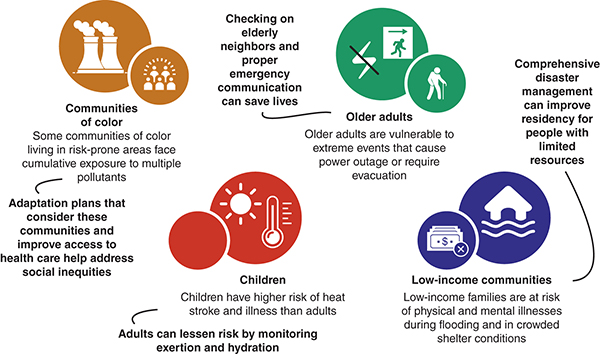
Long Description for Figure 3.5
Communities of color: Some communities of color living in risk-prone areas face cumulative exposure to multiple pollutants. Intervention: Adaptation plans that consider these communities and improve access to healthcare help address social inequities. Older adults: Older adults are vulnerable to extreme events that cause power outages or require evacuation. Interventions: Checking on elderly neighbors and proper communication can save lives. Children: Children have a higher risk of heat stroke and illness than adults. Interventions: Adults can lessen the risk by monitoring exertion and hydration. Low-income communities: Low-income communities of physical and mental illnesses during flooding and in crowded shelter conditions. Interventions: Comprehensive disaster management can improve residency for people with limited resources.
The Nurse’s Role in Social Determinants of Health and Vulnerable Populations
Addressing SDOH differences enables progress toward health equity, a state where every person can attain their highest level of health. Social determinants have been shown to have a greater influence on health than genetic factors or access to health care services. Indeed, SDOH, including the effects of centuries of racism, are key drivers of health inequities within communities of color. The impact is pervasive and deeply embedded in our society, creating inequities in access to various social and economic benefits, such as housing, education, wealth, and employment. These inequities put people at the lower end of the socioeconomic ladder at higher risk of poor health (CDC 2022e).
Nurses must focus on working with state and national agencies to ensure that resources reach those in need. Because SDOH constitute a multifaceted public health problem, nurses must collaborate with many sectors (e.g., transportation, education, housing, health care) and types of organizations (e.g., public agencies, private industry, community-based organizations).
Practice Application
➔ Setting the Scene
Health Care Disparities: Sharlene Adams Goes to Buy a Blood Pressure Cuff
Watch this video by scanning the QR code or visiting https://youtu.be/d6wH4nQVmhw

➔ Think About It
Consider Sharlene’s experience as showcased in the video.
- What factors did you notice that either contributed to or reduced Sharlene’s overall health?
- Of the factors you identified, how many are considered SDOH?
- What changes could the physician’s office make to make health care more accessible to Sharlene?
- What were the transportation barriers Sharlene experienced? Do you think this will reduce her health-seeking behaviors in the future? For example, future health screenings?
- What state or national policies can you identify that would contribute to or present barriers to Sharlene’s health if she lived in your neighborhood?
Additional Resources
CDC, National Environmental Public Health Tracking – Populations and Vulnerabilities
Center on Budget and Policy Priorities – A Quick Guide to SNAP Eligibility and Benefits
Healthy People 2030 – Environmental Conditions [Literature Summary]
PBS – Unnatural Causes … is inequality making us sick?
The State of Health Disparities in the United States [Book Chapter]
USDA, Food and Nutrition Service – A Short History of SNAP
Information on Unique, Vulnerable Populations
Communities of Color: Vulnerability and unmet health care needs. The influence of multiple risk factors [Article]
Persons with Disabilities: WHO – Disability
Older Persons: A framework for understanding old-age vulnerabilities [Article]
The HIV Community: KFF – The Global HIV/AIDS Epidemic
Persons Who Are Homeless: Loma Linda University Health, Institute for Health Policy and Leadership – Disparities in Health Care for the Homeless
Persons Who Are Incarcerated: Healthy People 2030 – Incarceration [Literature Summary]
LGBTQIA+ Community: Health People 2030 – LGBT
Economically Disadvantaged Children: OECD, Changing the Odds for Vulnerable Children: Building Opportunities and Resilience [Report]
Refugees/Immigrants: WHO – Refugee and migrant health
Persons Who Are Uninsured: Health Consequences of Uninsurance among Adults in the United States: Recent Evidence and Implications [Article]
References
Agency for Toxic Substances and Disease Registry. (2017). ToxFAQsTM for nitrate and nitrite. ATSDR. Retrieved August 11, 2022, from wwwn.cdc.gov/TSP/ToxFAQs/ToxFAQsDetails.aspx?faqid=1186&toxid=258
Agency for Toxic Substances and Disease Registry. (2022, August 10). Getting to Know GRASP. ATSDR. https://www.atsdr.cdc.gov/placeandhealth/getting_to_know_grasp.html
AJMC. (2006). Vulnerable populations: Who are they? Supplements and Featured Publications, 12(13 Suppl.). https://www.ajmc.com/view/nov06-2390ps348-s352
Bailey, K. T., Cook, J. T., Ettinger de Cuba, S., Casey, P. H., Chilton, M., Coleman, S. M., Cutts, D. B., Heeren, T. C., Rose-Jacobs, R., Black, M. M., & Frank, D. A. (2016). Development of an index of subsidized housing availability and its relationship to housing insecurity. Housing Policy Debate, 26(1), 172–187. https://doi.org/10.1080/10511482.2015.1015042
Balazs, C., & Ray, I. (2014). The drinking water disparities framework: On the origins and persistence of inequities in exposure. AJPH, 104(4). https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2013.301664
Berchick, E. R., Hood, E., & Barnett, J. C. (n.d.). Health insurance coverage in the United States: 2017. 44.
Brender, J. D., Maantay, J. A., & Chakraborty, J. (2011, December 1). Residential proximity to environmental hazards and adverse health outcomes. American Journal of Public Health, 101(S1), S37–S52. https://doi.org/10.2105/AJPH.2011.300183
Brummer, S., Reyes, I., Martin, M. L., Walker, L. U., & Heron, S. L. (2016). Racial/Ethnic health care disparities and inequities: Historical perspectives. In M. L. Martin, S. L. Heron, L. Moreno-Walton, & A. W. Jones (Eds.), Diversity and inclusion in quality patient care (pp. 11–21). Springer International Publishing. https://doi.org/10.1007/978-3-319-22840-2_2
Casey, J. A., Morello-Frosch, R., Mennitt, D. J., Fristrup, K., Ogburn, E. L., & James, P. (2017). Race/Ethnicity, socioeconomic status, residential segregation, and spatial variation in noise exposure in the contiguous United States. Environmental Health Perspectives, 125(7), 077017. https://doi.org/10.1289/EHP898
Centers for Disease Control and Prevention. (2019, March 8). Disability Impacts All of Us [Infographic]. www.cdc.gov/ncbddd/disabilityandhealth/infographic-disability-impacts-all.html
Centers for Disease Control and Prevention. (2020, December 1). Waterborne disease in the United States. www.cdc.gov/healthywater/surveillance/burden/index.html
Centers for Disease Control and Prevention. (2021a). Fast fact: Preventing bullying. www.cdc.gov/violenceprevention/youthviolence/bullyingresearch/fastfact.html
Centers for Disease Control and Prevention. (2021b, July 20). Unintended pregnancy. www.cdc.gov/reproductivehealth/contraception/unintendedpregnancy/index.htm
Centers for Disease Control and Prevention. (2022a, April 13). Racial/Ethnic disparities in pregnancy-related deaths—United States, 2007–2016 [Infographic]. https://archive.cdc.gov/#/details?url=https://www.cdc.gov/reproductivehealth/maternal-mortality/disparities-pregnancy-related-deaths/infographic.html
Centers for Disease Control and Prevention. (2022b, May 26). Water contamination and diseases. www.cdc.gov/healthywater/drinking/contamination.html
Centers for Disease Control and Prevention. (2022c, June 23). Pregnancy mortality surveillance system. www.cdc.gov/reproductivehealth/maternal-mortality/pregnancy-mortality-surveillance-system.htm
Centers for Disease Control and Prevention. (2022d, December 8). Social determinants of health. https://www.cdc.gov/about/sdoh/addressing-sdoh.html
Community Preventive Services Task Force. (2019, August 30). Mental health: Targeted school-based cognitive behavioral therapy programs to reduce depression and anxiety symptoms. The Community Guide. www.thecommunityguide.org/findings/mental-health-targeted-school-based-cognitive-behavioral-therapy-programs-reduce-depression-anxiety-symptoms
Feeding America. (2022). What is food insecurity? www.feedingamerica.org/hunger-in-america/food-insecurity
Joszt, L. (2018, July 20). 5 vulnerable populations in healthcare. AJMC. www.ajmc.com/view/5-vulnerable-populations-in-healthcare
Kaiser Family Foundation. (2018, May 10). Beyond health care: The role of social determinants in promoting health and health equity. www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/
Kann, L. (2018). Youth risk behavior surveillance—United States, 2017. MMWR Surveillance Summaries, 67. https://doi.org/10.15585/mmwr.ss6708a1
Magnan, S. (2017). Social Determinants of Health 101 for health care: Five plus five [Discussion paper]. NAM Perspectives. National Academy of Medicine. https://doi.org/10.31478/201710c
Mikati, I., Benson, A. F., Luben, T. J., Sacks, J. D., & Richmond-Bryant, J. (2018). Disparities in distribution of particulate matter emission sources by race and poverty status. American Journal of Public Health, 108(4), 480–485. https://doi.org/10.2105/AJPH.2017.304297
National Collaborating Centre for Determinants of Health. (2022). Glossary of essential health equity terms. https://nccdh.ca/learn/glossary/
Nemours Foundation. (2022). Reading and health are related. Nemours Children’s Reading BrightStart! www.readingbrightstart.org/articles-for-parents/reading-health-related/
Nethery, R. C., Mealli, F., Sacks, J. D., & Dominici, F. (2021). Evaluation of the health impacts of the 1990 Clean Air Act amendments using causal inference and machine learning. Journal of the American Statistical Association, 116(535), 1128–1139. https://doi.org/10.1080/01621459.2020.1803883
Office of Disease Prevention and Health Promotion. (2017). Reduce bullying of lesbian, gay, or bisexual high school students—LGBT-05. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/lgbt/reduce-bullying-lesbian-gay-or-bisexual-high-school-students-lgbt-05
Office of Disease Prevention and Health Promotion. (2022a). Economic stability. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/economic-stability
Office of Disease Prevention and Health Promotion. (2022b). Education access and quality. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/education-access-and-quality
Office of Disease Prevention and Health Promotion. (2022c). Environmental conditions. Healthy People 2030. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/environmental-conditions
Office of Disease Prevention and Health Promotion. (2022d). Food insecurity. Healthy People 2030. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/food-insecurity
Office of Disease Prevention and Health Promotion. (2022e). Health care access and quality. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/health-care-access-and-quality
Office of Disease Prevention and Health Promotion. (2022f). Housing instability. Healthy People 2030. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability
Office of Disease Prevention and Health Promotion. (2022g). High school graduation. Healthy People 2030. https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/high-school-graduation
Office of Disease Prevention and Health Promotion. (2022h). Increase the proportion of children whose family read to them at least 4 days per week—EMC-02. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/children/increase-proportion-children-whose-family-read-them-least-4-days-week-emc-02
Office of Disease Prevention and Health Promotion. (2022i). Neighborhood and built environment. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/neighborhood-and-built-environment
Office of Disease Prevention and Health Promotion. (2022j). Social and community context. Healthy People 2030. https://health.gov/healthypeople/objectives-and-data/browse-objectives/social-and-community-context
Office of Disease Prevention and Health Promotion. (2022k). Social determinants of health. Healthy People 2030. https://health.gov/healthypeople/priority-areas/social-determinants-health
Orr, M., Bove, F., Kaye, W., & Stone, M. (2002). Elevated birth defects in racial or ethnic minority children of women living near hazardous waste sites. International Journal of Hygiene and Environmental Health, 205(1–2), 19–27. https://doi.org/10.1078/1438-4639-00126
Robert Wood Johnson Foundation. (2002). A portrait of the chronically ill in America, 2001. https://folio.iupui.edu/bitstream/handle/10244/775/ChronicIllnessChartbook2001.pdf
Saha, S., Vaidyanathan, A., Lo, F., Brown, C., & Hess, J. J. (2021). Short term physician visits and medication prescriptions for allergic disease associated with seasonal tree, grass, and weed pollen exposure across the United States. Environmental Health, 20(1), 85. https://doi.org/10.1186/s12940-021-00766-3
Schaider, L. A., Swetschinski, L., Campbell, C., & Rudel, R. A. (2019). Environmental justice and drinking water quality: Are there socioeconomic disparities in nitrate levels in U.S. drinking water? Environmental Health, 18(1), 3. https://doi.org/10.1186/s12940-018-0442-6
Schanzer, B., Dominguez, B., Shrout, P. E., & Caton, C. L. M. (2007). Homelessness, health status, and health care use. American Journal of Public Health, 97(3), 464–469. https://doi.org/10.2105/AJPH.2005.076190
Tessum, C. W., Apte, J. S., Goodkind, A. L., Muller, N. Z., Mullins, K. A., Paolella, D. A., Polasky, S., Springer, N. P., Thakrar, S. K., Marshall, J. D., & Hill, J. D. (2019). Inequity in consumption of goods and services adds to racial–ethnic disparities in air pollution exposure. Proceedings of the National Academy of Sciences, 116(13), 6001–6006. https://doi.org/10.1073/pnas.1818859116
Turner, M. C., Krewski, D., Pope, C. A., Chen, Y., Gapstur, S. M., & Thun, M. J. (2011). Long-term ambient fine particulate matter air pollution and lung cancer in a large cohort of never-smokers. American Journal of Respiratory and Critical Care Medicine, 184(12), 1374–1381. https://doi.org/10.1164/rccm.201106-1011OC
United States Department of Agriculture. (2022). Definitions of food security. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/definitions-of-food-security/
United States Department of Agriculture, Economic Research Service. (2022). Key statistics & graphics. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/key-statistics-graphics/
U.S. Environmental Protection Agency. (2015, April 1). Overview of the Safe Drinking Water Act [Other policies and guidance]. https://www.epa.gov/sdwa/overview-safe-drinking-water-act
U.S. Global Change Research Program. (2016). The impacts of climate change on human health in the United States: A scientific assessment (pp. 1–312). https://health2016.globalchange.gov/executive-summary.html
Weinmeyer, R., Norling, A., Kawarski, M., & Higgins, E. (2017). The Safe Drinking Water Act of 1974 and its role in providing access to safe drinking water in the United States. AMA Journal of Ethics, 19(10), 1018–1026. https://doi.org/10.1001/journalofethics.2017.19.10.hlaw1-1710
Winny, A., Zhu, A., & Rogers, L. S. (2021, November 29). Public health in the field: The public health case for abortion rights. The Johns Hopkins University, Bloomberg School of Public Health. https://publichealth.jhu.edu/2021/public-health-in-the-field-the-public-health-case-for-abortion-rights
Woo, B., Kravitz-Wirtz, N., Sass, V., Crowder, K., Teixeira, S., & Takeuchi, D. T. (2019). Residential segregation and racial/ethnic disparities in ambient air pollution. Race and Social Problems, 11(1), 60–67. https://doi.org/10.1007/s12552-018-9254-0
Zierold, K. M., Hagemeyer, A. N., & Sears, C. G. (2020). Health symptoms among adults living near a coal-burning power plant. Archives of Environmental & Occupational Health, 75(5), 289–296. https://doi.org/10.1080/19338244.2019.1633992
