
6 | We Can Change Our Lives
Research Story: Pretend Play and Emotional Control in Young Children
Turns out, pretending to be a superhero or wizard is more than just child’s play. This kind of imaginative play can help kids learn to regulate emotions! Dr. Thalia R. Goldstein[2], a developmental psychologist at George Mason University, studied this exact thing with five-year-old children. She compared groups of children who participated in drama games, played with blocks, and listened to stories. Because everything is a learning opportunity when they are young, and children have diverse interests (i.e. they like to do many different things), five-year-olds were the perfect age group to introduce this theater intervention.
The Research Design
Goldstein wanted to examine how dramatic play might have a unique impact compared to other types of play with similar elements – in other words, are drama games beneficial in different ways than other play activities?
Goldstein hypothesized that the embodiment aspect of theatre and dramatic play that would cause changes for children. What does “embodying emotion” looks like? Goldstein gives the ‘right foot’ example: “Shift your right foot as if you were the most important and most powerful person in this room. How does your right foot feel different? Now I want you to imagine your right foot as if your favorite person in the whole world is about to walk through the door. What would your right food be doing right now?” That is an example of making an abstract emotion physical, or embodying it using your foot.
Try the “right foot” activity right now! How does your body change as you imagine different emotions?
Because Goldstein and her fellow researchers wanted to be able to make a causal claim, she used a randomized controlled field intervention. This means that they randomly assigned to one of three play groups (conditions), for eight weeks:
- Drama Games – games included acting out narratives with embodied emotions and characters with guidance around emotional embodiment.
- Block Play – guided block building, embodied action, no narrative, characters, or emotions.
- Story Time – stories that included characters and emotions, no emotional guidance or embodiment.
| Drama Games | Block Play | Story Time | |
|---|---|---|---|
| Group Interaction | Groups of 4, interacting | Groups of 4, interacting | Groups of 4, listening |
| Guidance | Guidance through games and emotions | Guidance for building and placing blocks | Guided reading with questions during books |
| Narrative/Character | Narrative and characters in games | No narrative or character | Narrative and characters in books |
| Emotions | Emotions in some games | No discussion of emotions | Emotions in some books |
| Embodiment | Embodied emotions and characters | Embodied actions in building | No embodiment |
Each of these conditions was designed to engage children in different aspects of theatre education. All three groups included four children interacting with each other along with some form of guidance, but the drama games condition was the only one with emotional guidance. The Story Time condition included stories with discussion about emotion, but no emotional embodiment and no physical action. The Block Play group included embodiment of action but no emotion or narrative. Comparison of the three groups can allow the researcher to come to stronger conclusions about the impact of drama games compared to simply observing a theater class.
The data collection phase of the study was double-blind, which means the researchers who observe and collect data are unaware of which kids were in what condition, or the point of the study overall. This helps minimize any experimenter bias. The data collection occurred before and after the eight week intervention and consisted of three parts:
- A Theory of Mind test
- A task where children had to give stickers away
- A task where the experimenter would ‘accidentally’ hurt themselves or drop something to see how the child would react. Would they cry? Or freeze?
Each of these tasks were designed to measure the extent to which children are prosocial and understanding of others. Goldstein also looked at how children understood their own emotions through several tasks. This included showing puppets that have different emotional responses and then asking the children which puppet was “most like” them.
The Research Results
Goldstein and her colleagues found no effect of the drama games condition on children’s engagement or understanding, but it did affect their emotional control. The children who were in the dramatic play group showed significantly less personal distress in a task than they did before the intervention started and compared to the children who were in the block play or story time groups. This was true for both their observed behavioral distress levels (such as crying or looking distressed) and the children’s self-report of their distress levels[4].
. Dramatic pretend play games uniquely improve emotional control in young children. Developmental science, 21(4), e12603\" id=\"return-footnote-4057-1\" href=\"#footnote-4057-1\" aria-label=\"Footnote 1\"><sup class=\"footnote\">[1]</sup></a> Y axis represents post-treatment values controlling for baseline.")
What do do these results tell us? What are the larger takeaways or theories we can draw from this experiment? Goldstein uses the analogy of a toolbox. She concludes that participating in theatre and playing drama games can add to an emotional toolbox for children learning to manage emotions. Each dramatic game or exercise may require a different tool or use a different toolbox; however they all are tools for emotion. Each tools theatre provides can be considered a strategy or skill for emotional regulation or emotional understanding that kids can then use outside of the game. The more children can learn about emotions, the more they can regulate them and understand them in others. Theatre games just help children gain those tools that they can then take with them in their toolbox into the real world.
Why is it be important for children to develop strategies for emotional regulation?
What are some future questions you might want to examine about theatre education, emotional regulation, or emotional understanding?
In what other ways could the knowledge gained through Dr. Goldstein’s theater games research improve the lives of children?
If drama games can help five-year-olds regulate emotions, could similar techniques help college students manage stress, anxiety, or interpersonal challenges?
Link to Learning: Video
If you would like to see Dr. Goldstein sharing her research with an Introductory Psychology class, watch this 24-minute video. She shares more information on this fascinating area of study.
KEY Integrative THEME:
Applying psychological principles can change our lives, organizations, and communities in positive ways.
Psychological principles don’t just live in research labs, libraries, or a scientist’s head —they shape the way we grow, work, and connect. Psychologists study how people make sense of the world, themselves, and each other. The resulting knowledge is communicated to a wide audience through books, blogs, news articles, movies and shows, parents, educators, and more. The psychological principles that make up our understanding of how people think, feel, and behave also help us understand what happens when things go wrong for people. We can then design ways to prevent things from going in an undesirable direction (such as laws or parenting practices), or interventions to change what happens when things go wrong (such as psychological treatment or new policies). Psychology is found in the world in expected places, such as a therapist’s or counselor’s office, and unexpected places, such as government or nature.
Let’s break down the theme into its’ components. Applying psychological principles can positively change:
- our personal lives, where it helps us understand and improve ourselves;
- our organizations, where it guides how we collaborate, lead, and thrive at work;
- and our communities, where it empowers us to address social challenges and build healthier, more equitable environments.
In this chapter, we’ll explore how psychology applies across these three key contexts. Dr. Thalia Goldstein’s work with young children and theater games demonstrates how psychological research can impact our lives. Dr. Reeshad Dalal and Dr. Seth Kaplan’s research on emotion regulation shows psychological principles at work in organizations, and Dr. Lisa Feldman Barrett’s research on the impact of words on our nervous system provides examples of how psychology can change our communities. Whether you’re navigating college life, preparing for a career, or thinking about your role in the world, psychology offers tools to help you change your life—and maybe even change the world.
You may have already found some applications for psychology in your work or personal life. What have you learned so far in this course that has been or might be useful?
LINK TO LEARNING
In the short video linked here, Garth Neufeld, a psychology professor at Cascadia College, explains the Key Theme.
Applying Psychological Principles In Our Organizations
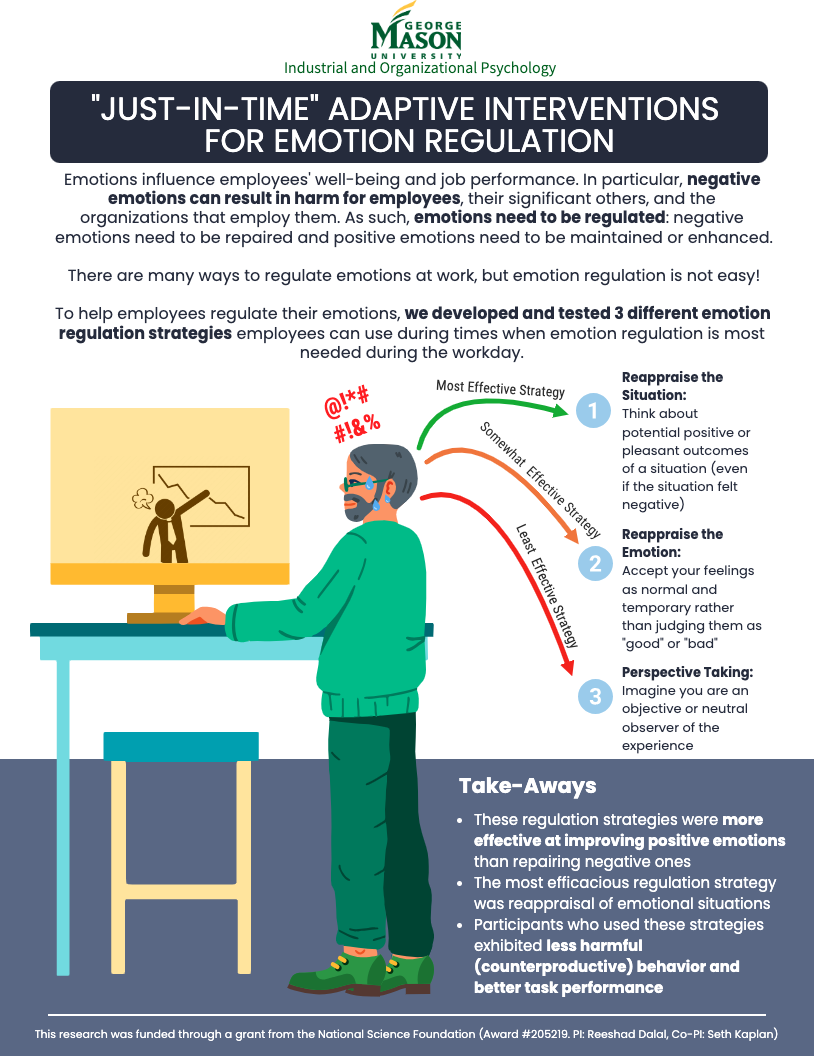
Just-in-Time Adaptive Interventions for Emotion Regulation
While theatre education can support children’s development of skills, adults too can practice and strengthen their emotion regulation abilities. In the labs of psychologists Dr. Reeshad Dalal[6] and Dr. Seth Kaplan[7] at George Mason University, researchers study emotion regulation from an industrial-organizational psychologist’s perspective: in the workplace. They created the infographic below (Fig. 6.3) to share their research. This infographic focuses on effective emotion regulation in the workplace, but, when you examine it, think about what these strategies might look like when applied to non-work situations as well. These tools can be used by anyone looking to manage their emotions.
Effective Strategies
Dalal and Kaplan found that the most effective strategy to help manage negative emotions and maintain positive ones was reappraising the situation. This means reframing the way you think about the situation even if it feels negative by looking for any positive outcomes from it. Another somewhat effective emotion regulation strategy was reappraising the emotion itself, meaning accepting whatever emotion you are feeling as normal instead of bad and reminding yourself the emotion won’t last forever. The last strategy, perspective-taking, was found to be the least effective of the three. Perspective-taking is when you try to separate yourself from the situation to be neutral. The researchers found these emotional regulation strategies to be helpful in the context of being more productive and having better performance at work.
Why do you think perspective-taking appears to be less effective than reappraisal?
These findings about effective emotion regulation were limited to the context of employee well-being and job performance, but the strategies can also be effective in other areas of life. Reappraising situations and emotions, and acting as a neutral observer are emotion regulation tools used in a variety of contexts. If the effectiveness of emotion regulation strategies was studied in a family or school context, do you think the results would be different? If so, which one do you think would be more effective?
Can you think of situations where you could use these tools?
It is important to note that emotion regulation is not emotion suppression – which is a coping strategy that can be unhealthy. When emotion is suppressed, the person does not identify, acknowledge, or express it and this can lead to negative physical and relational consequences. Our emotions are important signals that help us to function well – and should not be ignored. Emotion regulation on the other hand, is a skill that can help you manage negative emotions before they become overwhelming and overpower life experiences.
How is “reappraising the situation” different from “reappraising the emotion?” Why is this an important distinction?
applying psychological principles In the Community
How Emotions Are Made
Do you want to learn more about emotions and how they are made? The more you understand emotions, the more you may be able to further develop your regulation skills. The video below is a TED talk by Lisa Feldman Barrett, a psychologist and emotions researcher at Northeastern University who studies how the human brain, in conversation with the body and the world, regulates the body and creates mental events, such as episodes of emotion.
“Emotions are not made FOR you, they are made BY you.”
– Lisa Feldman Barrett
Dr. Barrett describes how understanding how emotions are created and experienced can help people regulate emotions like test anxiety – something that prevents some people from succeeding in college. Anxiety is an emotion that can often be refrained or appraised into another emotion, such as determination or excitement, and it is a learned skill. This understanding of how to reframe the interpretations of difficult emotions such as anxiety or nervousness, is another example of how we can change our lives using psychological science.
Link to Learning: Video
The video linked here comes with a warning: Once we understand that we have some control over our emotions, we then have more responsibility for how we feel and behave. You might need to give up some long-held assumptions about emotions, such as allowing other people to “make you feel” certain ways.
TED talk: You Aren’t at the Mercy of your Emotions, Your Brain Creates Them[8]
Did anything in this talk change how you might think about your emotions? How hard or easy do you think it is to regulate emotion?
Words Matter
Dr. Lisa Feldman Barrett also studies how words impact our brains and our bodies. Many species regulate each others’ nervous systems through sensory channels. For example, chemicals (such as pheromones), vocalizations, touch, smell, and vision are used by insects, mammals, and primates for communication that regulates nervous systems. Humans are unique in that they can use words as well as hugs, scents, and visuals. Our words can have a powerful impact on others – they can be a calming influence, then can trigger stress or fear, or they can affect trust and distrust. This is reflected in our nervous system, and can even be seen through brain scans. Words alone can influence activity in brain regions associated with movement, vision, and other bodily functions such as heart-rate, breathing, and the immune system.
LINK TO LEARNING
Listen to Dr. Feldman Barrett[9] describes this phenomenon in this short video.
Now that we understand the effect our words can have on other people’s nervous systems, we can reflect on the power we have to impact others’ experiences[10]. We don’t need a lot of money or expertise to use our words in an influential way in our communities daily.
For example, have you been told to always use “person-first language?” This is different from “first person.” For example, instead of referring to someone as “a homeless person,” (and thus centering homelessness), you would center the person by saying “a person experiencing homelessness.” The general recommendation is to center the humanity of a person rather than a characteristic, condition, or disability. However, it turns out that many people in the disability community, especially disability rights advocates, prefer identity first language. This is also true of many in the autistic community. Many people refer to themselves as “deaf” or “autistic,” rather than “a deaf person” or “a person with autism.”
There is no true consensus among these communities regarding person-first language, but the use of euphemisms such as “differently abled” or “special needs” that were created primarily by non-disabled people are often viewed as infantilizing or patronizing by disabled people. This is important information, because if someone insists on calling someone “special needs” and those words feel infantilizing to the person they are talking about, then that person’s nervous system will be stressed more than necessary. We can unknowingly cause distress in others with the words we choose to use. In fact, researchers have found that a positive identification with disability, across studies and populations, has been associated with better adaptation to disability (such as hope, optimism, quality of life), better engagement in care, lessened impact of ableism, and even lower depression and anxiety symptoms[11].
How can people outside of the disability community, such as teachers, classmates, neighbors, encourage positive identification with disability?
DEEPER DIVE: What is Disability?
The Center for Disease Control [12] defines disability as “ any condition of the body or mind that makes it more difficult for the person with the condition to do certain activities and interact with the world around them.”
The World Health Organization (WHO)[13] defines disability as resulting “from the interaction between individuals with a health condition, such as cerebral palsy, Down syndrome and depression, with personal and environmental factors including negative attitudes, inaccessible transportation and public buildings, and limited social support.”
Both definitions include three areas:
- Impairment
- Activity limitation
- Participation restrictions
This encompasses conditions that are both acquired (by accident or injury) or congenital (at birth) and can vary among several dimensions such as visibility, modality (physical, mental, sensory), and chronicity (temporary, chronic). Depending on who is included in the definition, estimates vary regarding the number of disabled people. The CDC estimates that 27% of adults in the U.S. have some type of disability, and the WHO estimates that 16% of the world’s population experiences disability.
Language and Disability: Relevance for the Psychology Student
So what do we do to avoid unknowingly stressing other people’s nervous systems? The best thing to do is to just ask a person how they want to be addressed and to be mindful of common phrases that are rooted in ableism and negative attitudes about disability. Language is important when it comes to attitude, and the avoidance of the word “disabled” has been seen as having negative consequences. In fact, there is a movement called #Saytheword that encourages people to add the word “disability” back into their language[14].
Adding the word “disability” back into our language as a valued social identity can improve our communities for disabled people. We know that the extent of disability experienced by an individual is significantly influenced by their environment. Inaccessible spaces can create obstacles that make engaging in basic activities such as healthcare, education, and employment difficult. In communities where spaces and experiences are built with accessibility in mind, disabled people will both have more opportunities and feel more like they belong in that community[15]. Accessibility ranges from physical access to spaces, (steps, ramps, elevators, wide enough doorways and walkways, seating) to digital access (text to speech, visibility of text and images, reading level, usability of websites and digital forms) and more. These considerations can change the environment so that the disability is not as much of a barrier.
What conditions would be necessary for a community to recognize disability as a valued social identity? What about other identities that are historically marginalized?
Traditional education spaces are environments that are often experienced as inaccessible. Recent estimates show that at least 12-13% of college students have a disability that impacts their learning. And yet, only about 6% of students access accommodations in the college classroom. Some students say they don’t access accommodations just as extended time on tests because they feel it is cheating – as do many non-disabled students. The reasoning behind classroom accommodations, however, is to level the playing field. If it takes me an hour to do something it only takes you a half hour to do, and I am only given half an hour, then I cannot demonstrate my knowledge or learn to my full capacity. You don’t need more than 30 minutes – in fact, providing more time for students who don’t need it does not improve test scores. Next time you hear someone saying that it’s not okay to access extended time accommodations, could you speak up and try to change their mind?
If you, your family or friends, or your classmates are disabled, this conversation might seem relevant. But even if none of the above are true, the psychology student needs to pay attention to language and accessibility. The American Psychological Association has guidelines on inclusive language to be used in writing and other forms of communication in psychology, and there are basic accessibility considerations for anything you create that will be “consumed” by the general public. These should be consulted when completing assignments and projects in your classes. For example, the following list from the APA guidelines suggests terms to avoid and alternatives. Note that many of these options use person-first language; the distinction between person-first and identity-first is less important here. The focus is on traditionally used terms that should be avoided and what to use instead.
| Terms to avoid | Suggested alternative |
| special needs, handi-capable, differently abled | person with a disability, disabled person |
| physically/mentally challenged | person with intellectual disabilities, physically disabled |
| visually challenged | blind |
| person who is deaf | Deaf person or Deaf-Blind |
| wheelchair-bound, confined to a wheelchair | person who uses a wheelchair, wheelchair user |
| mentally ill, crazy, insane, mental defect, suffers from or is afflicted with [condition] | person living with a mental illness or with a mental health disorder; person with a diagnosis of a mental illness/mental health disorder/behavioral health disorder |
| drug user/abuser, addict | person who uses drugs, person with substance use disorder |
| alcoholic, alcohol abuser | person with alcohol use disorder;person in recovery from substance use/alcohol disorder |
| relapsed | returned to use |
| homeless people, the homeless, transient populations | people who are not securely housed, or experiencing homelessness or food/housing insecurity; people experiencing unsheltered homelessness; guests who are accessing homeless services |
| prostitute | person who engages in sex work; sex worker (abbreviated as SWer) |
| prisoner, convict | person who is/has been incarcerated |
| slave | person who is/was enslaved |
Link to Learning: Website
DID YOU KNOW?
Connections and Summary
In this chapter you have read examples of the key theme at work. Dr. Goldstein’s lab used scientific methods to determine what kinds of play can help children to develop crucial emotion regulation skills. This research was published and so that others can continue to study this phenomenon, and so that it teachers and parents can develop activities for children to support their development (applying psychological principles can change our lives). The Industrial-organizational psychologists Dr. Dalal and Dr. Kaplan studied strategies for emotion regulation in the workplace, and created an infographic to share their results with the general public. When people practice these strategies, it enhances the overall working environment (applying psychological principles can change our organizations). The American Psychological Association has published guidelines to encourage the use of language that will reduce the emotional distress that can be caused by harmful words. Additionally, our communities can be enhanced through the recognition of disability as a valued social identity (applying psychological principles can change our communities in positive ways).
Exercises
- What are some other topics you would like to see discussed through the lens of this key theme?
- Can you take another key theme and look at these topics through that lens?
- Is there an area you would like to know more about regarding how psychological principles can change our lives, communities, and organizations in positive ways?
- How have you seen psychology in action in your world?
- Goldstein, T. R., & Lerner, M. D. (2018). Dramatic pretend play games uniquely improve emotional control in young children. Developmental science, 21(4), e12603 ↵
- Psychology | Faculty and Staff: Thalia R Goldstein.” Psychology, psychology.gmu.edu/people/tgoldste. ↵
- Goldstein, T. R. (2018). Developing a Dramatic Pretend Play Game Intervention. American Journal of Play, 10(3), 290-308. ↵
- Goldstein, T. R., & Lerner, M. D. (2018). Dramatic pretend play games uniquely improve emotional control in young children. Developmental science, 21(4), e12603. ↵
- Goldstein, T. R., & Lerner, M. D. (2018). Dramatic pretend play games uniquely improve emotional control in young children. Developmental science, 21(4), e12603 ↵
- Psychology | Faculty and Staff: Reeshad S. Dalal.” Psychology, psychology.gmu.edu/people/rdalal. Accessed 1 Aug. 2024. ↵
- Faculty and Staff: Seth Kaplan.” Psychology, 2019, psychology.gmu.edu/people/skaplan1. ↵
- Barrett, Lisa Feldman. “You Aren’t at the Mercy of Your Emotions -- Your Brain Creates Them. Www.ted.com, 2 Jan. 2018 ↵
- Next Big Idea Club. “The Power of Words: How They Shape Your Mind and Body.” YouTube, 1 Dec. 2020, youtu.be/XKgLvSXTL9U?si=4qSY8meimmh8RqqT. Accessed 1 Aug. 2024. ↵
- Martin H. Teicher, M.D., Ph.D., Jacqueline A. Samson, Ph.D., Yi-Shin Sheu, M.A., Ann Polcari, R.N., Ph.D., and Cynthia E. McGreenery. Hurtful Words: Association of Exposure to Peer Verbal Abuse With Elevated Psychiatric Symptom Scores and Corpus Callosum Abnormalities Published Online:1 Dec 2010 https://doi.org/10.1176/appi.ajp.2010.10010030 ↵
- Dunn & Burcaw 2013, Forber-Pratt, Lyew, Mueller & Samples, 2017 ↵
- Centers for Disease Control and Prevention. Disability and Health Data System (DHDS) [Internet]. Available from: http://dhds.cdc.gov ↵
- World Health Organization, International Classification of Functioning, Disability and Health (ICF) Geneva: 2001, WHO. ↵
- Andrews, E. E., Forber-Pratt, A. J., Mona, L. R., Lund, E. M., Pilarski, C. R., & Balter, R. (2019). #SaytheWord: A disability culture commentary on the erasure of “disability”. Rehabilitation Psychology, 64(2), 111–118. https://doi.org/10.1037/rep0000258 ↵
- Dunn & Burcaw 2013, Forber-Pratt, Lyew, Mueller & Samples, 2017 ↵
- Telhan, R., McNeil Ba, K. M., Lipscomb-Hudson, A. R., Guobadia, E. L., & Landry, M. D. (2020). Reckoning With Racial Trauma in Rehabilitation Medicine. Archives of physical medicine and rehabilitation, 101(10), 1842–1844. https://doi.org/10.1016/j.apmr.2020.07.001 ↵
This is a specialty area focused on the study and application of psychological knowledge and skills on behalf of people with chronic health conditions and disabilities. The goal is to maximize health, independence, functional abilities, and social roles - such as relationships, parenting, and employees - across the lifespan. Training in this area is in clinical, developmental, or social psychology, and sometimes other domains as well. Read more about this important area at the APA Division 22 Website.
