
Chapter 14: Health and Wellness
Anxiety, Depression, And Self-Directed Violent Behavior
Anxiety, Depression, And Self-Directed Violent Behavior
Developmental models of anxiety and depression treat adolescence as an important period, especially in terms of the emergence of differences and in prevalence rates that persist through adulthood (Rudolph, 2009). Although the rates vary across specific anxiety and depression diagnoses, rates for some disorders are markedly higher in adolescence than in childhood or adulthood. For example, 18.2% of adults in the United States report experiencing anxiety symptoms (Terlizzi & Zablotsky, 2024), while the same can be said for 25% of adolescents (Liu et al, 2019). Adolescents are also slightly more likely to experience depression (25.2%; Psychogiou et al., 2024) compared to adults (Terlizzi & Zablotsky, 2024) [Note that rates of anxiety and depression increased substantially during and immediately following the COVID-19 pandemic (Psychogiou et al., 2024). Therefore, these statistics may fluctuate noticeably in the coming years.] Rates of self-directed violence are also higher among teens and college students (23-33%) (Wachter-Morris & Wester, 2020; Wester et al., 2018), followed by adults (4.4%; Harford et al., 2019).
Anxiety
Occasional anxiety is an expected part of life. You might feel anxious when faced with a problem, before taking a test, or when making an important decision. But anxiety disorders involve more than temporary worry or fear. For a person with an anxiety disorder, the anxiety does not go away and can get worse over time. The symptoms can interfere with daily activities such as job performance, school work, and relationships.
The wide variety of anxiety disorders differ by the objects or situations that induce them but share features of excessive anxiety or worry about a variety of things. Fear and anxiety can cause significant problems in areas of their life, such as social interactions, school, and work. Anxiety also manifests in physiological and psychological responses, such as feeling restless, fatigued, difficulty concentrating, irritability, muscle tension, and sleep problems.
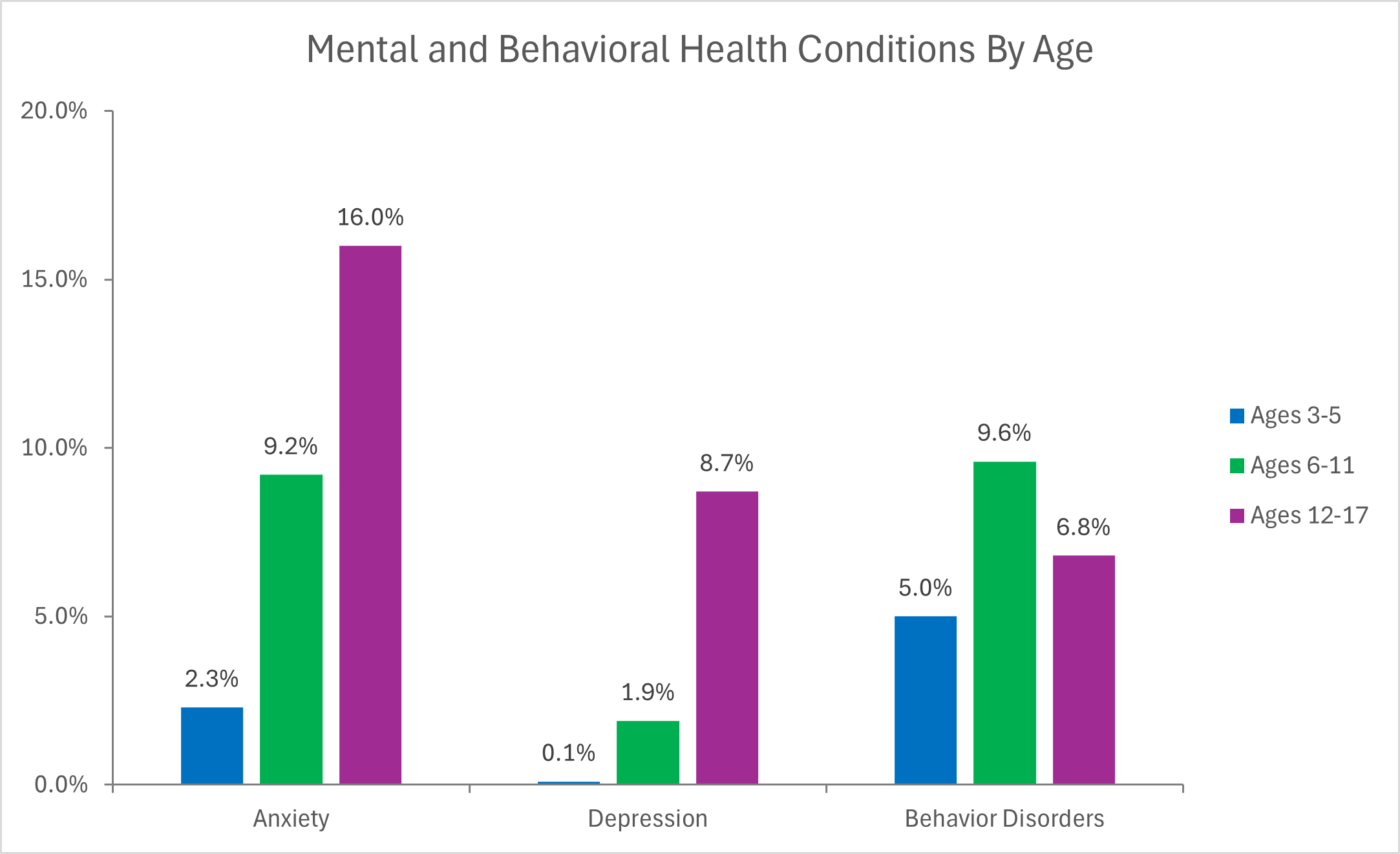
The following data pertains to the compiling of statistics for any anxiety disorder including, panic disorder, generalized anxiety disorder, agoraphobia, specific phobia, social anxiety disorder, post-traumatic stress disorder, obsessive-compulsive disorder, and separation anxiety disorder. Approximately 30% of children and adolescents have an anxiety disorder (CDC, 2025). The prevalence of any anxiety disorder among children and adolescents was slightly higher for females (12%) than for males (9%).
Anxiety disorders are generally treated with psychotherapy, medication, or both. Psychotherapy or “talk therapy” can help people with anxiety disorders. To be effective, psychotherapy must be directed at the person’s specific anxieties and tailored to his or her needs. Medication does not cure anxiety disorders but can help relieve symptoms. Medication for anxiety is prescribed by doctors, such as a psychiatrist or primary care provider. The most common classes of medications used to combat anxiety disorders are anti-anxiety drugs (such as benzodiazepines), antidepressants, and beta-blockers. Some people with anxiety disorders might benefit from joining a self-help or support group and sharing their problems and achievements with others. Talking with a trusted friend or member of the clergy can also provide support, but it is not necessarily a sufficient alternative to care from a doctor or other health professional. Stress management techniques and meditation can help people with anxiety disorders calm themselves and may enhance the effects of therapy. Research suggests that aerobic exercise can help some people manage their anxiety; however, exercise should not take the place of standard care, and more research is needed.
The Prevalence of Mental Illness in youth
Video 14.4. Teen Brains are Not Broken
Depression
Sadness is something we all experience. It is a normal reaction to a loss or a setback, but it usually passes with a little time. Depression is different. Depression (major depressive disorder) is a medical illness that can interfere with a person’s ability to handle daily activities, such as sleeping, eating, or managing responsibilities. Depression is common, but that doesn’t mean it isn’t serious. Well-meaning friends or family members may try to tell someone with depression to “snap out of it,” “just be positive,” but depression is not a sign of weakness or a character flaw. Many people with depression need treatment to get better.
Depression is characterized by feelings of deep sadness and hopelessness that disrupts all normal, regular activities. However, teens may not identify feelings of sadness and instead report feeling more irritable and angry. Often, when depressed, people feel worthless and excessively guilty. They withdraw from activities that they normally enjoy and spend more time alone. Changes in appetite and sleeping habits (more or less than normal) are common. People with depression may experience fatigue, having low energy, and also feel restless. Physical aches and pains with no associated reason may occur, like muscle, stomach, or headaches. Cognitive functioning, such as attention, concentration, memory, and decision-making, may be impaired. And while not necessary for a depression diagnosis, thoughts of death or suicide may be an issue.
Teens with depression may sulk, get into trouble at school, be negative and irritable, and feel misunderstood. It can be difficult to determine whether an adolescent is depressed or just “being a teenager.” Consider how long the symptoms have been present, how severe they are, and how different the teen is acting from his or her usual self. Teens with depression may also have co-occurring disorders such as anxiety, eating disorders, or substance abuse.
The prevalence of major depressive episodes among U.S. adolescents in 2017 was estimated at 3.2 million adolescents aged 12 to 17 in the United States with at least one major depressive episode. This number represented 13.3% of the U.S. population aged 12 to 17. The prevalence of major depressive episodes was higher among adolescent females (20.0%) compared to males (6.8%). The prevalence of major depressive episodes was highest among adolescents reporting two or more races (16.9%).
Causes of depression include many factors, such as genetics and early childhood experiences that predate adolescence, but puberty may push vulnerable children, especially girls, into despair. During puberty, the rate of major depression more than doubles to an estimated 13%, affecting about one in five girls and one in ten boys. The gender difference occurs for many reasons, including biological and cultural (Uddin et al., 2010).
Developmental models focus on interpersonal contexts in both childhood and adolescence that foster depression and anxiety (e.g., Rudolph, 2009). Family adversity, such as abuse and parental psychopathology during childhood, sets the stage for social and behavioral problems during adolescence. Adolescents with such problems generate stress in their relationships (e.g., by resolving conflict poorly and excessively seeking reassurance) and select into more maladaptive social contexts (e.g., “misery loves company” scenarios in which depressed youths select other depressed youths as friends and then frequently co-ruminate as they discuss their problems, exacerbating negative affect and stress). These processes are intensified for girls compared with boys because girls have more relationship-oriented goals related to intimacy and social approval, leaving them more vulnerable to disruption in these relationships. Anxiety and depression then exacerbate problems in social relationships, which in turn contribute to the stability of anxiety and depression over time.
Depression, even in the most severe cases, can be treated. The earlier that treatment can begin, the more effective it is. Depression is usually treated with medications, psychotherapy, or a combination of the two. An estimated 19.6% received care by a mental health professional alone, and another 17.9% received combined care by a mental health professional and medication treatment. Treatment with medication alone was the least common (2.4%). Approximately 60.1% of adolescents with major depressive episodes did not receive treatment.
Antidepressants are medicines that treat depression. They may help improve the way the brain uses certain chemicals that control mood or stress. Trying several different antidepressant medications may be necessary before finding the one that improves symptoms and has manageable side effects. Antidepressants take time – usually 2 to 4 weeks – to work, and often, symptoms such as sleep, appetite, and concentration problems improve before mood lifts, so it is important to give medication a chance before reaching a conclusion about its effectiveness.
Several types of psychotherapy (also called “talk therapy” or, in a less specific form, counseling) can help people with depression. Examples of evidence-based approaches specific to the treatment of depression include cognitive-behavioral therapy (CBT), interpersonal therapy (IPT), and problem-solving therapy. CBT can help an individual with depression change negative thinking and interpret the environment and interactions in a positive, realistic way. IPT is designed to help an individual understand and work through troubled relationships or major issues that may cause depression or make it worse.
Teenagers usually rely on parents, teachers, or other caregivers to recognize their suffering and get them the treatment they need. Many teens don’t know where to go for mental health treatment or believe that treatment won’t help. Others don’t get help because they think depression symptoms may be just part of the typical stress of school or being a teen. Some teens worry about what other people will think if they seek mental health care.
Self-Directed Violence
Self-directed violence (SDV) encompasses a range of violent behaviors, including acts of fatal and nonfatal suicidal behavior, and non-suicidal self-injury (i.e., behaviors where the intention is not to kill oneself, as in self-mutilation). Recognizing signs of self-directed violence and interventions to help people engaging in this behavior can save a life and help get them treatment.
Non-suicidal self-injury (NSSI), also referred to as self-harm or self-mutilation, is a “deliberate, self-inflicted injury without suicidal intent and not for socially sanctioned purposes (such as tattoos or piercings). NSSI is most often associated with ‘cutting,’ but means of self-harm often also include scratching, pinching, punching oneself, banging objects with the intention of injury, biting, tearing of the skin, or burning. The location of the injury may also be an indicator of the severity of the psychological disturbance. Injuries to the face, eye, jugular, or genitals may be more concerning. Although not a suicide attempt, NSSI is associated with suicide and can result in an accidental fatality (Whitlock, 2010).
The average age of the first NSSI is between 11 and 15 years old. The prevalence of at least one incident NSSI is estimated to be 12-37% in high school populations and 12 to 20% in late adulthood and early adulthood cohorts, with 6-7% of adolescents reporting repetitive NSSI in the last year. Of those reporting repetitive incidents, 40% reported stopping the behavior within a year of starting, and the vast majority (79.8%) stopped within five years (Whitlock, 2010).
While we might presume that NSSI behavior is associated with mental illness, like depression and anxiety, that is not always the case. Forty-four percent of people who engage in common NSSI do not have any co-morbidity. This type of NSSI includes self-injurious behaviors that are (1) compulsive or ritualistic (like trichotillomania), (2) episodic or occasional, with no identification as a person who self-harms, and (3) repetitive with a self-harming identity. Common NSSI can be mild, moderate, or severe, depending on the severity of the injuries (Whitlock, 2010).
The reasons for NSSI are psychological, social, and biological and often stem from a history of childhood adversity, comorbid psychological disorders, and emotional dysregulation. Psychological reasons are the most common and involve reducing psychological pain, expressing distress, and distracting oneself from other negative stimuli. Fewer teens report social reasons for NSSI, such as seeking attention or copying peers. Social factors, like peer reinforcement of the behavior, can increase the likelihood of repetitive NSSI. Those reporting “getting a rush” or “feeling normal” from NSSI may have biological reasons for the behavior. These individuals may have chronically low levels of certain neurotransmitters in their brains. The neurochemical response to injury may bring these neurotransmitter levels to a more normal level and help them regulate emotions. This may be the reason that some people are dependent on NSSI (Whitlock, 2010).
The correlation between NSSI and suicide-related behaviors is well known, but the nature of that relationship is rather paradoxical. Moving from NSSI to suicide-related behaviors may appear to be a predictable progression in severity; without intervention, those engaged in NSSI may get worse and eventually become suicidal. However, experts agree that NSSI may actually help alleviate the distress that could lead to suicide-related behavior, at least temporarily. NSSI could be a tool for coping with distress and avoiding suicide (Whitlock, 2010).
In 2017, suicide was the second leading cause of death for people aged 10-19. After a stable period from 2000 to 2007, suicide death rates for teens are now increasing. Distressing thoughts about killing oneself become most common at about age 15 and can lead to a variety of suicide-related behaviors (Castellví et al., 2017).
Suicide-related behaviors include the following:
- Suicide: Death caused by self-directed injurious behavior with any intent to die.
- Suicide attempt: A non-fatal self-directed potentially injurious behavior with any intent to die as a result of the behavior. A suicide attempt may or may not result in injury.
- Suicidal ideation: Thinking about, considering, or planning for suicide.
Suicide-related behavior is complicated and rarely the result of a single source of trauma or stress. Youth who are at increased risk for suicide-related behavior are dealing with a complex interaction of multiple relationships (peer, family, or romantic), mental health, and school stressors. Often, people who engage in suicide-related behavior experience overwhelming feelings of helplessness and hopelessness. Involvement with bullying behavior is one stressor that may significantly contribute to feelings of helplessness and hopelessness that raise the risk of suicide.
Youth are at higher risk for suicide-related behaviors if they experienced violence, including child abuse, bullying, or sexual violence, and cannot cope with problems in healthy ways and solve problems peacefully. Teens with disabilities, learning differences, sexual/gender identity differences, or cultural differences are often most vulnerable to being bullied. Teens who report frequently bullying others are at high, long-term risk for suicide-related behavior. Youth who report both being bullied and bullying others (sometimes referred to as bully-victims) have the highest rates of negative mental health outcomes, including depression, anxiety, and thinking about suicide.
The behaviors listed below may be signs that someone is thinking about suicide.
- Talking about wanting to kill themselves or making a plan to kill themselves
- Talking about feeling empty, hopeless, or having no reason to live
- Talking about great guilt or shame
- Talking about feeling trapped or feeling that there are no solutions
- Feeling unbearable pain (emotional pain or physical pain)
- Talking about being a burden to others
- Using alcohol or drugs more often
- Acting anxious or agitated
- Withdrawing from family and friends
- Changing eating and/or sleeping habits
- Showing rage or talking about seeking revenge
- Taking great risks that could lead to death, such as driving extremely fast
- Talking or thinking about death often
- Displaying extreme mood swings, suddenly changing from very sad to very calm/happy
- Giving away important possessions
- Saying goodbye to friends and family
- Putting affairs in order, making a will
If these warning signs apply to you or someone you know, get help as soon as possible, particularly if the behavior is new or has increased recently. Call the National Suicide Prevention Lifeline (Lifeline) at 1-800-273-TALK (8255), or text the Crisis Text Line (text HELLO to 741741). Both services are free and available 24 hours a day, seven days a week. The following recommendations are five action steps to help someone in emotional pain:
- ASK: “Are you thinking about killing yourself?” It’s not an easy question, but studies show that asking at-risk individuals if they are suicidal does not increase suicides or suicidal thoughts.
- KEEP THEM SAFE: Reducing a suicidal person’s access to highly lethal items or places is an important part of suicide prevention. While this is not always easy, asking if the at-risk person has a plan and removing or disabling the lethal means can make a difference.
- BE THERE: Listen carefully and learn what the individual is thinking and feeling. Research suggests acknowledging and talking about suicide may reduce rather than increase suicidal thoughts.
- HELP THEM CONNECT: Save the National Suicide Prevention Lifeline’s (988 or 1-800-273-TALK (8255)) and the Crisis Text Line’s number (741741) in your phone, so it’s there when you need it. You can also help make a connection with a trusted individual like a family member, friend, spiritual advisor, or mental health professional.
- STAY CONNECTED: Staying in touch after a crisis or after being discharged from care can make a difference. Studies have shown the number of suicide deaths goes down when someone follows up with the at-risk person.
Check Your Understanding.
a medical illness that can interfere with a person’s ability to handle daily activities, such as sleeping, eating, or managing responsibilities
