
16 Chapter 16 The Neurological Exam
By Krishnan Prabhakaran
Motivation.
Head trauma and concussions can happen to adults and children alike. There are countless different ways in which traumatic brain injuries can occur: a direct physical blow to the head, falling on the ground, or a car accident – among many other possibilities.
However, concussions can also happen even when there is no direct blow to the head. In some cases, a concussion can even happen with simple sudden movements or jolts, and these “minor” concussions often go undetected and undiagnosed. Even when caused by a direct blow to the head, most concussions don’t lead to a loss of consciousness and are left untreated.
Each concussion is different, and not everyone exhibits the same symptoms. The best way to recognize and assess the extent of a concussion is to get a neurological exam by a clinical neuroscience practitioner. Here is what you can expect.
There are many types of neurological assessments that licensed practitioners will do with their patients. Neurological assessments are the most effective way of recognizing and analyzing concussions. In most cases, doctors will use a special brain imaging techniques like CT or MRI scans to look for brain abnormalities.
Unfortunately, CT & MRI scans are often ineffective in recognizing concussions because most lesions in the brain caused by a head trauma are too small to be identified by these types of scans. This is why neurological assessments are a fundamental tool in understanding the effects of a head trauma as a whole and can evaluate just how extensive the damage is.
Common neurological assessments include:
- Assessing mental capacity & status
- Pupil size assessment
- Sensory exams
- Pupil reactivity assessment
- Blood pressure measurement
- Handgrip strength assessment
- Motor function & balance exercises
- Pulse measurements
- Respiration assessment
In most cases, these neurological assessments last around an hour. They are non-invasive and don’t involve any brain stimulants. Sometimes people might not feel any initial symptoms after a traumatic brain injury. This is why it’s generally a good idea to visit a practitioner and go through the examination to make sure everything is in good order.
Learning Objectives
Upon completion of the work in this chapter students should be able to:
- Describe the mental status exam and perform simple tests to determine brain function
- Perform sensory and motor exams (e.g. sight, eye movement) to determine cranial nerve function
- Utilize sensory and motor exams to determine the health of spinal cord functions
- Perform coordination and gait exams as indicators of cerebellar integration of neuronal function
Background.
A. Overview of the Neurological Exam
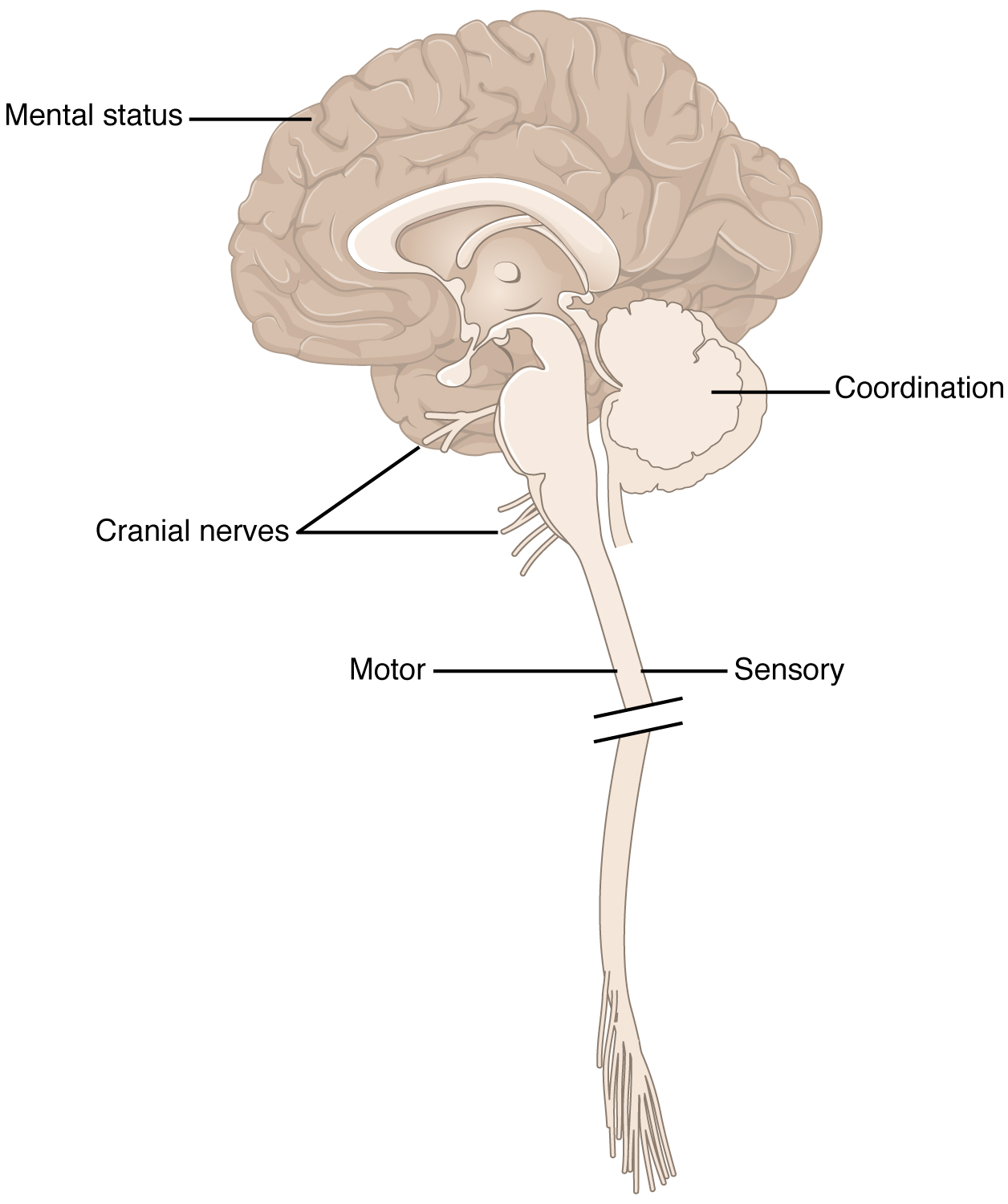
The neurological exam is a clinical assessment tool used to rapidly determine which specific parts of the CNS are affected by damage or disease. The exam can be broken down into the following subsets:
- Mental Status Exam = assesses the higher cognitive functions such as memory, orientation, and language.
- Cranial Nerve Exam = tests the function of the 12 cranial nerves and, therefore, the central and peripheral structures associated with them.
- The Sensory Exam = tests the sensory functions associated with the spinal nerves.
- The Motor Exam = tests the motor functions associated with the spinal nerves
- The Coordination Exam = tests the ability to perform complex and coordinated movements. The Gait Exam = specifically assesses the motor function of walking and can be considered part of the coordination exam because walking is a coordinated movement.
B. Causes of Neurological Deficits
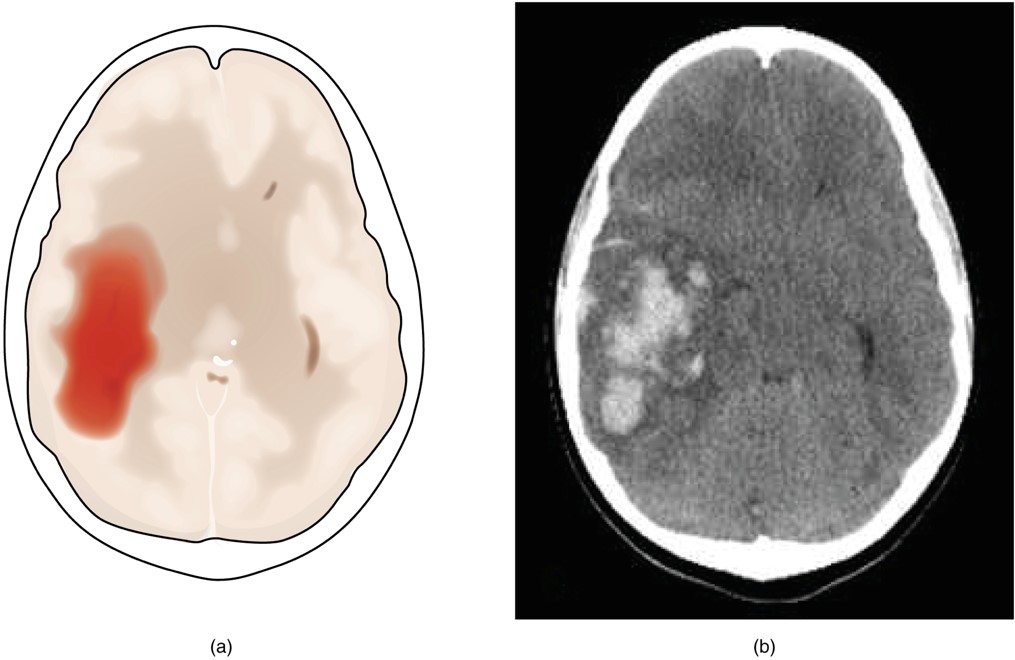
1. Stroke also called CVA cerebrovascular accident= the loss of blood flow to a part of the brain. There are different types of stroke as indicated below.
- Ischemic stroke = the loss of blood flow to an area because vessels are blocked or narrowed. This is often caused by an embolus (blood clot or fat deposit), thickening of the vessel wall or drop in blood volume = hypovolemia. Transient ischemic attack (TIA) is similar to an ischemic stroke, but symptoms are resolved within 24 hours.
- Hemorrhagic stroke = bleeding into the brain because of a damaged blood vessel. Accumulated blood fills in a region of the cranial vault and presses against the tissue in the brain. This pooling blood causes secondary symptoms such as loss of function, pressure on neighboring arteries resulting in a larger damage area, potentially compromising the blood-brain barrier resulting in additional fluid on brain = edema.
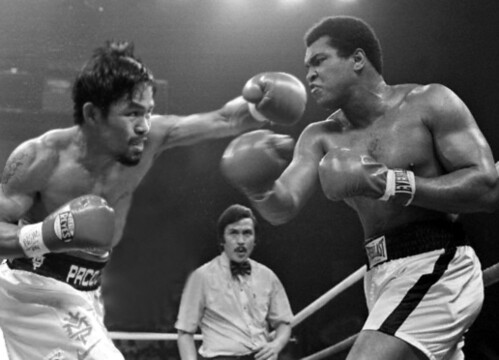
2. Blunt force trauma can cause neurological deficits (Figure 16.1).
3. Neurodegenerative diseases, developmental, and other disorders
- Alzheimer’s disease = a progressive disorder characterized by the loss of higher cerebral functions and is the most common cause of senile dementia or senility. Symptoms may appear at 50 – 60 years or age. Associated with ACh shortages, shrinkage of the gyri, and formation of neural tangles among the CNS neurons and Alzheimer plaques within the cerebrum.
- Parkinson’s disease = neurodegenerative disorder of the substantia nigra resulting in decreased production of dopamine. The basal nuclei become more active, which raises skeletal muscle tone and produces rigidity and stiffness. Individuals, with Parkinson disease have difficulty starting voluntary movements, because opposing muscle groups do not relax; they must be overpowered. Once a movement is underway, every aspect must be voluntarily controlled through intense effort and concentration.
- Huntington’s disease = genetic disorder of the basal nuclei result in too much movements. occurs 1 in 20,000 births and is the result of a dominant gene located on chromosome 4. Causes a progressive neurological degeneration leading to death within 20 years from onset of symptoms. Symptoms show in 20s or 30-40 years of age.
- Amyotrophic Lateral Sclerosis (ALS) = progressive, degenerative disorder that affects the motor neurons in the spinal cord, brain stem, and cerebral hemispheres. The degeneration affects both upper and lower motor neurons. Because a motor neuron and its dependent muscle fibers are so intimately related, the destruction of the CNS neurons causes atrophy of the associated skeletal muscles.
- Rabies – A bite from a rabid animal injects the rabies virus into the peripheral tissues, where virus particles quickly enter the synaptic knobs. Retrograde flow then carries the virus into the CNS, with potential fatal consequences. Many toxins (including heavy metals), some pathogenic bacteria, and other viruses also bypass CNS defenses by exploiting axoplasmic transport.
- Multiple Sclerosis (MS) = autoimmune disease causing deterioration of the myeline that affects axons in the optic nerve, brain, and spinal cord. MS results in paralysis and potentially death. The disorder is progressive and functional impairment increases following each new incident. Women are 1.5 times more likely to have MS than men.
- Cerebral Palsy – refers to a number of disorders that affect voluntary motor performance; they appear during infancy or childhood and persist throughout the life of affected individuals. The cause may be trauma associated with premature or unusually stressful birth, maternal exposure to drugs, or a genetic defect that causes the improper development of motor pathways.
- Referred Pain – the sensation of pain in a part of the body other than its actual source.
C. Mental Status Exam – Background
This exam probes the functions of the cerebral cortex.
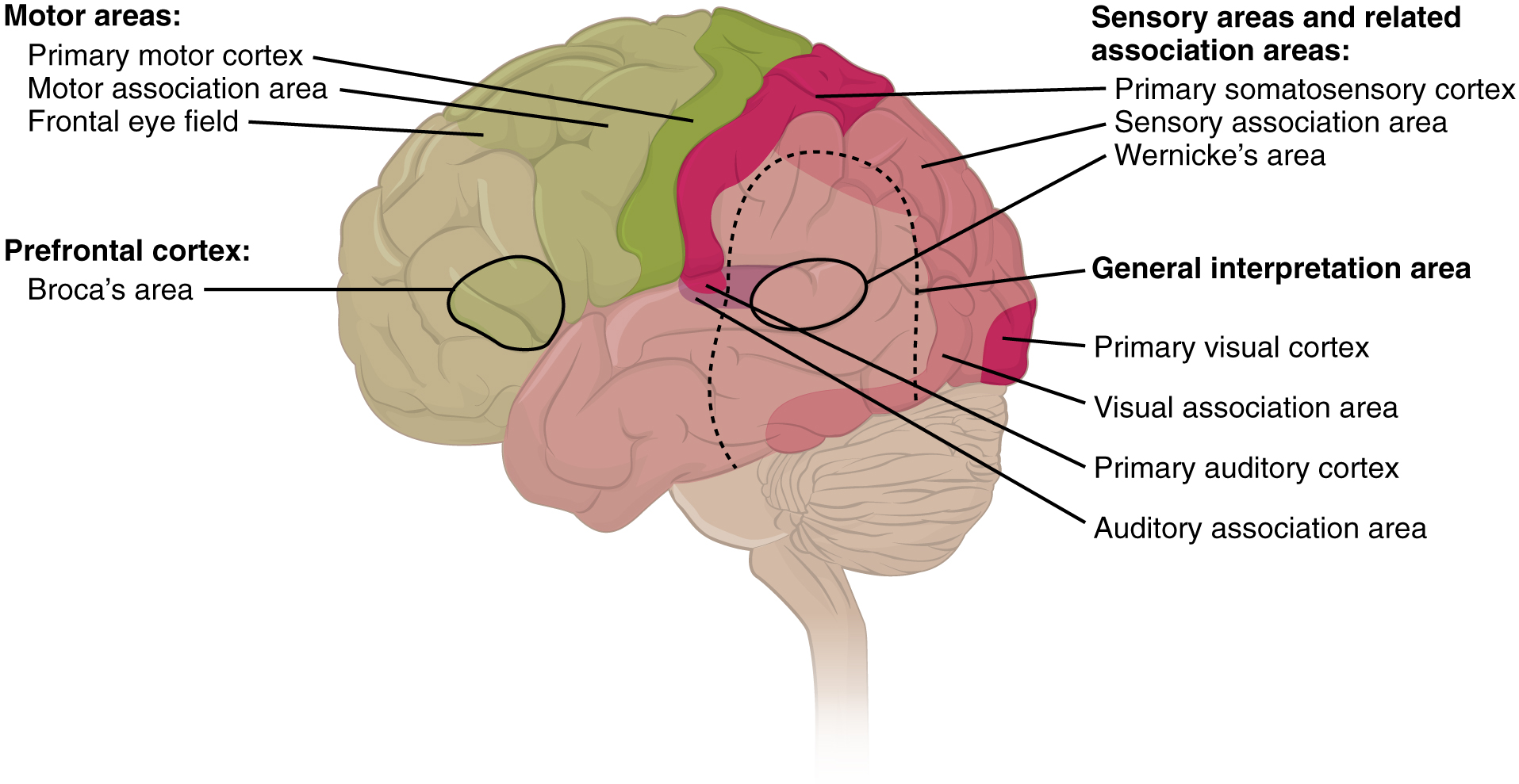
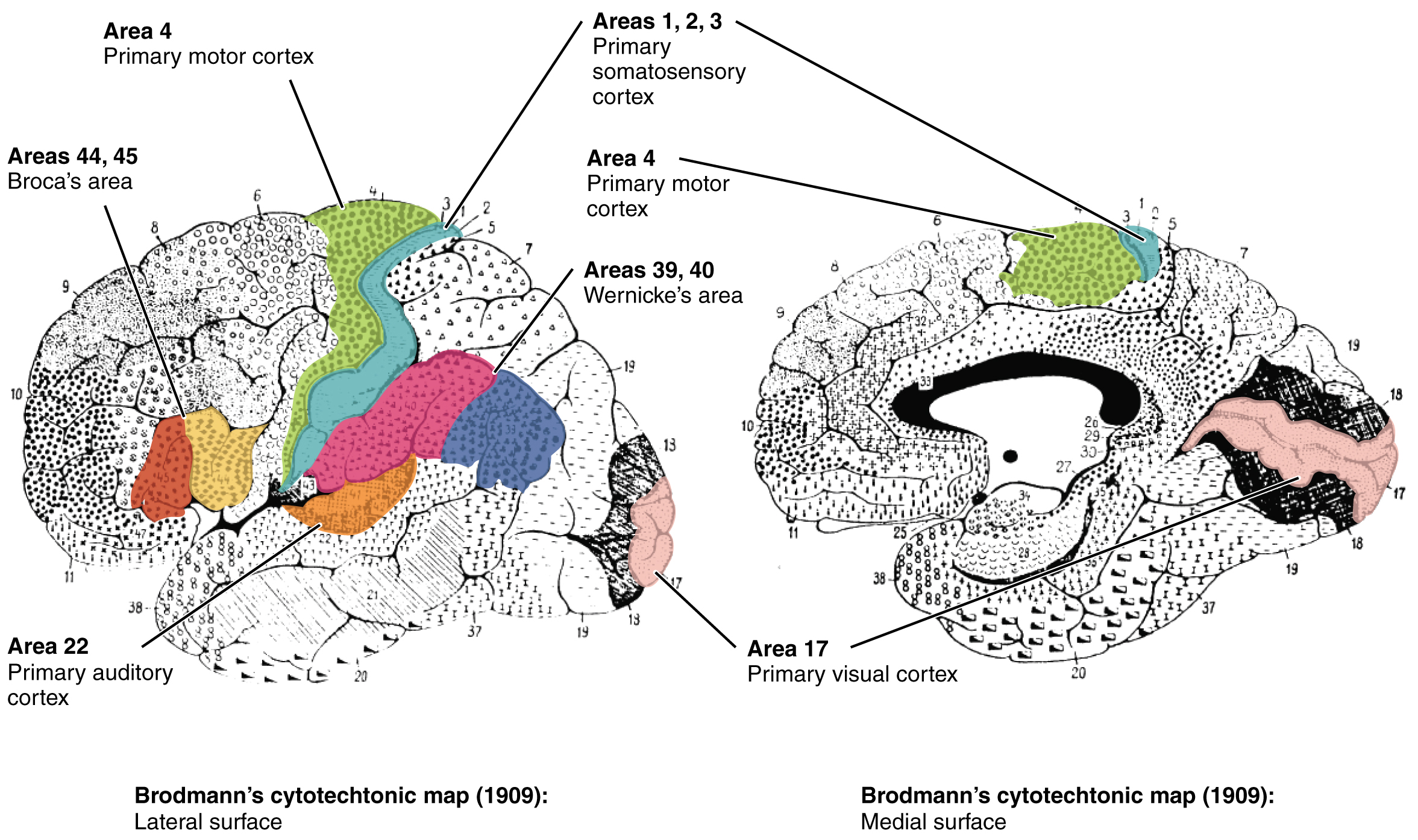
- Primary = The primary cortical areas are where sensory information is initially processed, or where motor commands emerge to go to the brain stem or spinal cord.
- Association = Association areas are adjacent to primary areas and further process the modality-specific input.
- Integration areas = Multimodal integration areas are found where the modality-specific regions meet; they can process multiple modalities together or different modalities on the basis of similar functions, such as spatial processing in vision or somatosensation. Example of picking up a glass and based on what is in it determines what body movements we make.
D. Cranial Nerve Exam – Background
The Cranial Nerve Exam allows directed tests of forebrain and brain stem structures.
- The olfactory nerve (CN I) receives sense of smell.
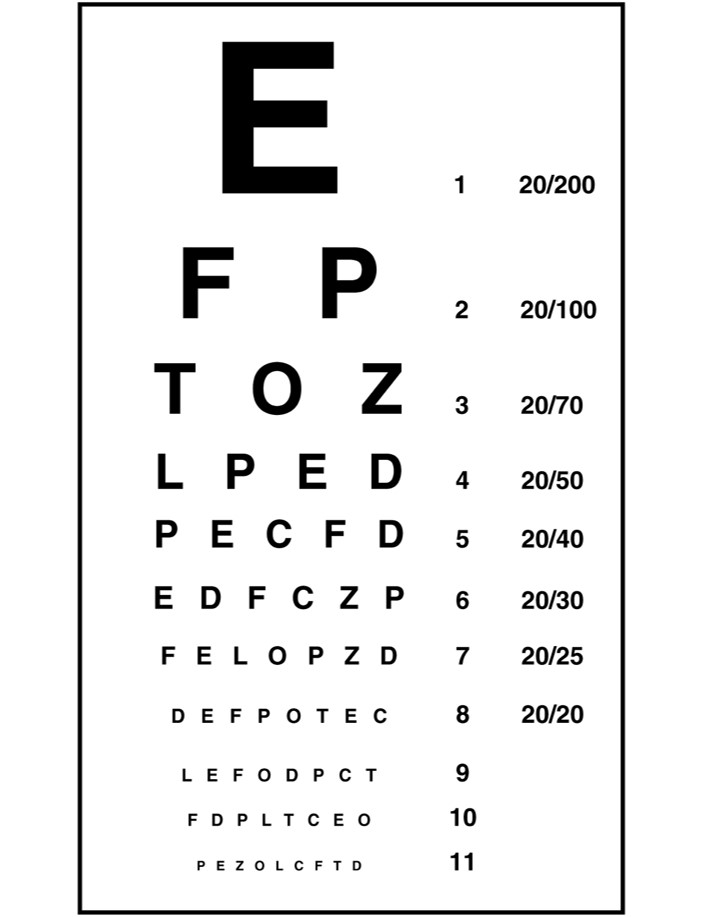
- Optic nerve (CNII) receives sense of vision. Testing vision relies on the tests that are common in an optometry office such as the Snellen chart. Additionally, testing the extent of the visual field means that the examiner can establish the boundaries of peripheral vision. Furthermore, physical inspection of the optic disk, or where the optic nerve emerges from the eye, can be accomplished by looking through the pupil with an ophthalmoscope.
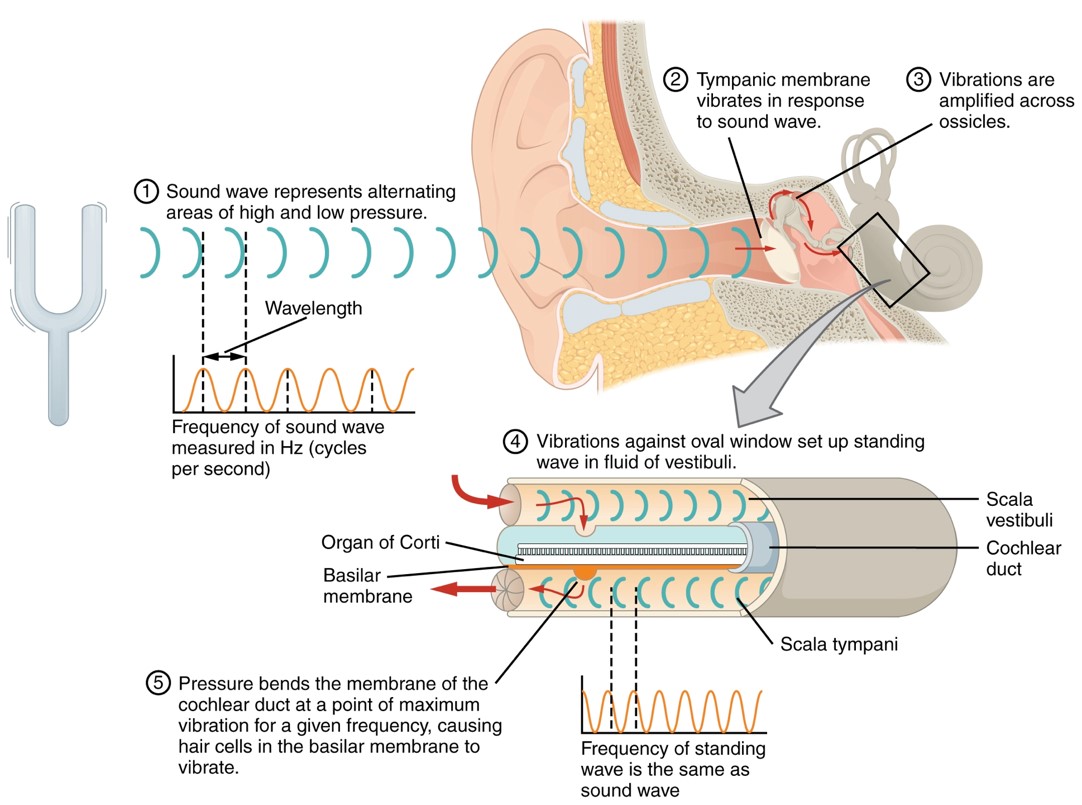
- Vestibulocochlear nerves (CN VIII) receives sense of equilibrium and hearing. Problems with balance, such as vertigo, and deficits in hearing may both point to problems with the inner ear.
- Conductive hearing= relies on vibrations being conducted through the ossicles of the middle ear.
- Sensorineural hearing = relies on the transmission of sound stimuli through the neural components of the inner ear and cranial nerve.
- Taste sensation is relayed to the brain stem through fibers of the facial (CN VII) and glossopharyngeal nerves (CN IX) and the vagus nerve (X).
- The trigeminal nerve (CN V) is a mixed nerve that carries the general somatic senses from the head, similar to those coming through spinal nerves from the rest of the body. The primary sensory subtest for the trigeminal system is sensory discrimination.
- Gaze Control. The three nerves that control the extraocular muscles are the:
- Oculomotor (CN III) – Movement of eyelid and eyeball (via superior rectus, inferior rectus, medial rectus, and inferior oblique), shape of lens, contracts pupil size
- Trochlear (CN IV) – Movement of eye by the superior oblique
- Abducens (CN VI) – Movement of the eyeball by the lateral rectus
- Gaze Control. The types of movements that are tested are:
-
- Saccades = rapid, conjugate movements of the eyes to survey a complicated visual stimulus, or to follow a moving visual stimulus.
- Diplopia, or double vision, as the two eyes are temporarily pointed at different stimuli.
- Convergence = when the two eyes move to look at something closer to the face, they both adduct. To keep the stimulus in focus, the eye also needs to change the shape of the lens, which is controlled through the parasympathetic fibers of the oculomotor nerve. The change in focal power of the eye is referred to as accommodation. Accommodation ability changes with age; focusing on nearer objects, such as the written text of a book or on a computer screen, may require corrective lenses later in life. Coordination of the skeletal muscles for convergence and coordination of the smooth muscles of the ciliary body for accommodation are referred to as the accommodation–convergence reflex.
-
- A crucial function of the cranial nerves is to keep visual stimuli centered on the fovea of the retina. The vestibulo-ocular reflex (VOR) coordinates all of the components, both sensory and motor, that make this possible
- Nerves of the Face and Oral Cavity. The facial (CN VII) and glossopharyngeal (CN IX) nerves convey gustatory stimulation to the brain. The hypoglossal nerve is the motor nerve that controls the muscles of the tongue, except for the palatoglossus muscle, which is controlled by the vagus nerve (CN X). There are two sets of muscles of the tongue. The extrinsic muscles of the tongue are connected to other structures, whereas the intrinsic muscles of the tongue are completely contained within the lingual tissues.
- Facial nerve = controls muscles controlling facial expressions, secretion of saliva by the submandibular and sublingual glands and tears by the lacrimal gland, and sensory function for taste from the anterior 2/3 of the tongue
- Glossopharyngeal = controls secretion of saliva by the parotid glands, elevation of pharynx during swallowing, and taste.
- Aguesia = loss of taste
- Bells Palsy = characterized by muscle weakness that causes one half of the face to droop. Bell’s palsy may be a reaction to a viral infection and usually resolves on its own within six months.
- Motor Nerves of the Neck. The accessory nerve (CN XI) innervates the sternocleidomastoid and trapezius muscles.
E. Sensory and Motor Exams – Background
Sensory Modalities and Location
- Somatic senses are incorporated mostly into the skin, muscles, or tendons, whereas the visceral senses come from nervous tissue incorporated into the majority of organs such as the heart or stomach.
- The somatic senses are those that usually make up the conscious perception of the how the body interacts with the environment.
- The visceral senses are most often below the limit of conscious perception because they are involved in homeostatic regulation through the autonomic nervous system.
- Testing of the senses begins with examining the regions known as dermatomes that connect to the cortical region where somatosensation is perceived in the postcentral gyrus.
Muscle Strength and Voluntary Movement
- The skeletomotor system is largely based on the simple, two-cell projection from the precentral gyrus of the frontal lobe to the skeletal muscles. Outputs from the frontal lobe synapse at the spinal ventral horn motor neurons (Upper Motor Neuron UMN and Lower Motor Neuron LMN) before projecting to the skeletal muscle.
- The lack of muscle tone, known as hypotonicity or flaccidity, may indicate that the LMN is not conducting action potentials that will keep a basal level of acetylcholine in the neuromuscular junction.
- Diseases that result in UMN lesions include cerebral palsy or MS, or it may be the result of a stroke.
Reflexes
- For the arm, the common reflexes to test are of the biceps, brachioradialis, triceps, and flexors for the digits. For the leg, the knee-jerk reflex of the quadriceps is common, as is the ankle reflex for the gastrocnemius and soleus.
- Plantar reflex tests for the Babinski sign on the basis of the extension or flexion of the toes at the plantar surface of the foot. The plantar reflex is commonly tested in newborn infants to establish the presence of neuromuscular function. To elicit this reflex, an examiner brushes a stimulus, usually the examiner’s fingertip, along the plantar surface of the infant’s foot. An infant would present a positive Babinski sign, meaning the foot dorsiflexes and the toes extend and splay out. As a person learns to walk, the plantar reflex changes to cause curling of the toes and a moderate plantar flexion.
Comparison of Upper and Lower Motor Neuron Damage
- Many of the tests of motor function can indicate differences that will address whether damage to the motor system is in the upper or lower motor neurons. Signs that suggest a UMN lesion include muscle weakness, strong deep tendon reflexes, decreased control of movement or slowness, pronator drift, a positive Babinski sign, spasticity, and the clasp-knife response. Spasticity is an excess contraction in resistance to stretch. It can result in hyperflexia, which is when joints are overly flexed. The clasp-knife response occurs when the patient initially resists movement, but then releases, and the joint will quickly flex like a pocket knife closing.
- A lesion on the LMN would result in paralysis, or at least partial loss of voluntary muscle control, which is known as paresis. The paralysis observed in LMN diseases is referred to as flaccid paralysis, referring to a complete or partial loss of muscle tone, in contrast to the loss of control in UMN lesions in which tone is retained and spasticity is exhibited. Other signs of an LMN lesion are fibrillation, fasciculation, and compromised or lost reflexes resulting from the denervation of the muscle fibers
F. Coordination and Gait Exams – Background
Locations and Connections of the Cerebellum
- Cerebellum = accounts for 11% of the brain’s mass.
- The cerebellum functions in the coordination and modulation of motor command from the cerebral cortex and maintaining balance and equilibrium.
- The cerebellum is partially hidden by the cerebral hemispheres and is the second largest structure in the brain.
- The cerebellum is separated from the cerebrum by the transverse fissure.
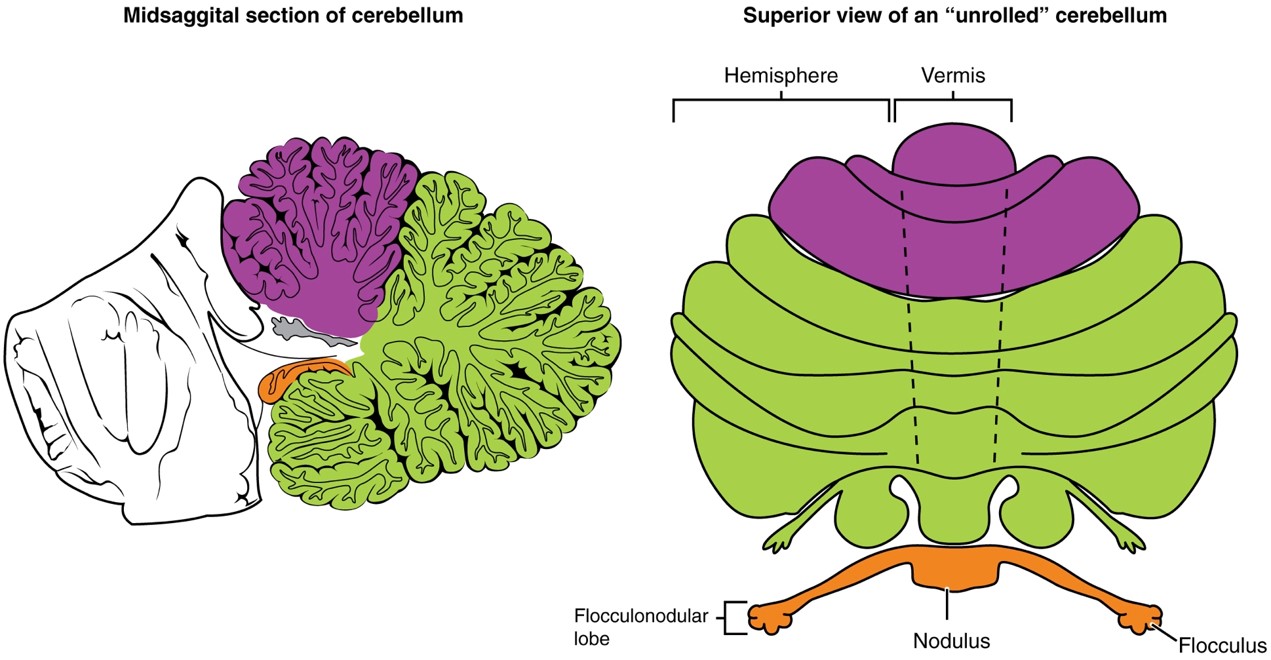
- The cerebellum also possesses fold-like wrinkles called folia, is divided into two hemispheres, and further subdivided into lobes: the anterior lobe and posterior lobe.
- The two cerebellar hemispheres are separated by the vermis while the anterior and posterior lobes are separated by the primary fissure.
- The white matter of the cerebellum is called the arbor vitae and is surrounded by gray matter called the cerebellar cortex.
Coordination and Alternating Movement
- Testing for cerebellar function is the basis of the coordination exam. The subtests target appendicular musculature, controlling the limbs, and axial musculature for posture and gait. The assessment of cerebellar function will depend on the normal functioning of other systems addressed in previous sections of the neurological exam. Motor control from the cerebrum, as well as sensory input from somatic, visual, and vestibular senses, are important to cerebellar function.
- The subtests that address appendicular musculature, and therefore the lateral regions of the cerebellum, begin with a check for tremor.
- The check reflex depends on cerebellar input to keep increased contraction from continuing after the removal of resistance. The patient flexes the elbow against resistance from the examiner to extend the elbow.
Pre-Laboratory Questions
1.The neurological exam is an assessment tool used to rapidly determine which parts of the CNS are affected using 5 different exams ________________, ________________, ________________, ________________, and ________________.
2. Bleeding into the brain due to a damaged blood vessel is called a _____________ ___________.
3. ___________ disease is a progressive degenerative disease caused by degeneration of the substantia nigra resulting in stooping, rigidity, stiffness and tremors.
4. The three cranial nerves that transmit gustatory impulses are the _________________, ________________, and __________________________.
5. All three nerves transmitting gustatory impulses travel through the ___________________ and is why gag and vomiting reflexes are triggered when we experience something distasteful.
6. The primary gustatory area is located in which part of the brain? __________________________________
7. The loss of taste sensation is called _________________________________________________________.
8. Olfactory sensation reaches the brain via which cranial nerve? ____________________________________
9. Brain disorders can distort the sense of smell so that olfactory hallucinations occur. Transient __________ _____________________ occur in some epileptics just before they have a seizure.
10. The __________ test uses a tuning fork placed on the top of the skull to determine sensorineural hearing.
Exercises
- Exercise 1 The Mental Status Exam
- Exercise 2 The Cranial Nerve Exam
- Exercise 3 The Sensory and Motor Exams
- Exercise 4 Coordination and Gait Exams
Exercise 1 The Mental Status Exam
Required Materials
- Your classmates
- Dull pointer such as a pen cap
- Any object for recognizing by touch
Procedure
In this exercise, you will use some of the commonly used practices to test for cognitive abilities. You can practice asking these questions and noting the answers using one of your group mates as a “patient”. Use pen and paper (or iPad notebook etc.) to record your questions and answers. At the end of the section, describe your conclusions.
- Testing Orientation and Memory
- Orientation = the patient’s awareness of his or her immediate circumstances.
- Awareness of time = date.
- Ask the question:“Do you know what day it is?”
- Record the answer here:_________________
- Awareness of place = location of where they are and why as well as who they are.
- Ask the question: “Do you know where you are?”
- Record the answer here:____________
- Ask the question: “What is your name?”
- Record the answer here: “Who is the current president?”
- Memory = the patient’s ability to recall information. Memory is largely a function of the temporal lobe, along with structures beneath the cerebral cortex such as the hippocampus and the amygdala. Amnesia can be defined as losing memories of events of the past retrograde amnesia or inability to make future memories anterograde amnesia.
- Short term memory can be assessed using the three-word test. Patients are given three words and after a brief time period are asked to recall the three words. Ask a question to test short term memory.
- Record your question here:__________________________________
- Record the answer here:____________________________________
- Orientation = the patient’s awareness of his or her immediate circumstances.
- Testing Language and Speech
- Language is at the core of what it means to be self-aware. Asking the patient to perform a set of actions can assess the ability to understand language. Often, language deficits can be determined without specific subtests; if a person cannot reply to a question properly, there may be a problem with the reception of language. Aphasia is the loss or speech or language.
- Ask the question: “Use you right pointer finger to touch the tip of your nose and then your left elbow.”
- Record your observation:__________________________
- Speech
- Broca’s area = responsible for speech production. Expressive aphasia = speech production is compromised leading to broken or haulted speech with incorrect grammar usage.
- Does your classmate have broken or haulted speech?_______
- Wernicke’s area = responsible for processing or understanding speech. Receptive aphasia = patients do not understand what is said to them or what they are saying even when they are talking.
- Does your classmate have difficulty with this? _______
- Conduction aphasia = patient’s inability to connect understanding of speech to production of speech. Symptoms include inability to faithfully repeat spoken language.
- Record a question to test this: _________________________
- Record the answer here:______________________________
- Language is at the core of what it means to be self-aware. Asking the patient to perform a set of actions can assess the ability to understand language. Often, language deficits can be determined without specific subtests; if a person cannot reply to a question properly, there may be a problem with the reception of language. Aphasia is the loss or speech or language.
- Testing Sensorium. The parts of the brain involved in reception and interpretation of sensory stimuli. From the primary cortical areas of the somatosensory, visual, auditory, and gustatory senses to the association areas that process information in these modalities, the cerebral cortex is the seat of conscious sensory perception. Two subtests assess specific functions of these cortical areas.
-
- Praxis = a practical exercise in which the patient performs a task completely on the basis of verbal description without any demonstration from the examiner. For example, the patient can be told to take their left hand and place it palm down on their left thigh, then flip it over so the palm is facing up, and then repeat this four times.
-
- Record a question to test this:_____________________
- Record the answer here:_________________________
-
- Gnosis – sensory perception involving two processes.
-
- Stereognosis = involves the naming of objects strictly on the basis of the somatosensory information that comes from manipulating them with their eyes closed, e.g. by touch
- Find an object and ask your classmate to identify it just by touch. What is the object you chose?___________
- Record the response here:______________
- Graphesthesia = recognize numbers or letters written on the palm of the hand with a dull pointer, such as a pen cap.
- Trace a letter on your classmate’s palm. Explain what you did exactly: _______________________
- Record the response here:________________________
- Stereognosis = involves the naming of objects strictly on the basis of the somatosensory information that comes from manipulating them with their eyes closed, e.g. by touch
-
- Praxis = a practical exercise in which the patient performs a task completely on the basis of verbal description without any demonstration from the examiner. For example, the patient can be told to take their left hand and place it palm down on their left thigh, then flip it over so the palm is facing up, and then repeat this four times.
- Testing Judgment and Abstract Reasoning. Making judgments and reasoning in the abstract are necessary to produce movements as part of larger responses. The prefrontal cortex involved in this process is related to personality.
- Ask questions that requires this and record the answers. Then repeat the process with another classmate. Think about the similarities and differences of their answers and what this reflects about their personality:
- Question: “When your alarm goes off, do you hit the snooze button or jump out of bed?”
- Record the answer here: ______________
- Question: Is 10 extra minutes in bed worth the extra rush to get ready for your day?
- Record the answer here:_____________
- Question: Will hitting the snooze button multiple times lead to feeling more rested or result in a panic as you run late? _____________
- Record the answer here:____________
- Ask questions that requires this and record the answers. Then repeat the process with another classmate. Think about the similarities and differences of their answers and what this reflects about their personality:
- Conclusions: List the conclusions from your mental status exam of your classmate regarding the following:
- Orientation:______
- Memory:_______
- Language:______
- Speech:______
- Sensorium:______
- Judgement and abstract reasoning:______
Exercise 2 The Cranial Nerve Exam
Required Materials
- Your classmates
- Eye Exam or Snellen Chart
- Tuning forks
- Cotton tipped applicator
- Pen or pencil
Procedure
Here you will practice testing the functions of some of the cranial nerves. Follow the instructions for testing or try to come up with ways in which you could given the definitions of nerve function. Record what you tested and the results.
- Testing the Optic nerve (CNII). Use the Snellen chart (Figure 16.6) to test visual acuity. Ask your classmate to stand 20 feet from the chart and read it. What is the smallest letter line they can read? What is their visual acuity? Record that number here:_____________
- Testing the Vestibulocochlear nerves (CN VIII):
- Conductive hearing test. The Rinne test.
- Place a vibrating tuning fork on the mastoid process of your classmate.
- Ask your classmate to tell you when the sound produced from this is no longer present.
- Then move the fork immediately to just next to the ear canal so the sound travels through the air.
- If the sound is not heard through the ear, meaning the sound is conducted better through the temporal bone than through the ossicles, a conductive hearing deficit is present.
- Does your classmate hear the tuning fork after it is placed next to the ear canal conducting through air?_______
- Sensorineural hearing test. The Webber test.
- Place a vibrating tuning fork at the top of the skull of your classmate, allowing the sound of the tuning fork to reach both inner ears by travelling through bone.
- Ask your classmate if the sound appears equally loud in both ears. Record their answer here: __________________
- With unilateral conductive hearing loss the tuning fork sounds louder in the ear with hearing loss. This is because the sound of the tuning fork has to compete with background noise coming from the outer ear, but in conductive hearing loss, the background noise is blocked in the damaged ear, allowing the tuning fork to sound relatively louder in that ear. With unilateral sensorineural hearing loss, however, damage to the cochlea or associated nervous tissue means that the tuning fork sounds quieter in that ear.
- Does your classmate have unilateral conductive hearing loss? Explain._____________
- Testing the trigeminal nerve (CN V) for sensory discrimination.
- Use a cotton-tipped applicator, which is cotton attached to the end of a thin wooden stick.
- Snap the wood of the applicator so that a pointed end is opposite the soft cotton-tipped end.
- The cotton end provides a touch stimulus, while the pointed end provides a painful, or sharp, stimulus.
- While your classmate’s eyes are closed, touch the two ends of the applicator to the classmate’s face, alternating randomly between them. Ask the classmate to identify whether the stimulus is sharp or dull.
- Was your classmate able to distinguish between the dull cotton and sharp wooded point? Explain what this means. _______
- Testing the Motor Nerves of the Neck. The accessory nerve (CN XI) innervates the sternocleidomastoid and trapezius muscles.
- Ask your classmate to flex head forward and side to side. What is your observation? Which muscle’s function does this test? Record your observation and conclusion here:______________
- Ask your classmate to extend and hyperextend the head as well as shrug the shoulders. What do these three motions test? i.e. which muscle’s function? What is your observation and conclusion? Record it here:______
Exercise 3 The Sensory and Motor Exams
Required Materials
- Your classmates
- Cotton tipped applicator
- Reflex hammer
Procedure
Where indicated, follow the instructions to test a subset of sensory and motor functions below:
- Testing Sensory Responses.
- To test the sensory fields, a simple stimulus of the light touch of the soft end of a cotton-tipped applicator is applied at various locations on the skin.
- Use the cotton tip, apply a soft touch on different parts of the body of your classmate and record your results here:
- Part 1 touched:______
- Response:_____
- Part 2 touched:_____
- Response:_____
- Part 3 touched:_____
- Response:_____
- Part 4 touched:_____
- Response:_____
- Part 5 touched:_____
- Response:______
- Is there one part of the skin that is more sensitive than another? Explain.___________
- Testing Lower Motor Neuron (LMN) Function. The lack of muscle tone may indicate that the LMN is not conducting action potentials to maintain muscle.
- Test your classmate’s muscle strength. Ask your classmate to lift the arm, while you are pushing down on it.
- Is your classmate able to resist? What does this mean about their LMN function? Explain.______
- Testing Upper Motor Neuron Function. Use the pronator drift test.
- Ask your classmate to to extend both arms in front of the body with the palms facing up.
- While keeping the eyes closed, is your classmate able to keep both arms extended in front of the body? _______
- If the “patient” unconsciously allows one or the other arm to slowly relax, toward the pronated position, this could indicate a failure of the motor system to maintain the supinated position. Does your classmate have this failure? What does this mean about their UMN? Explain._________-
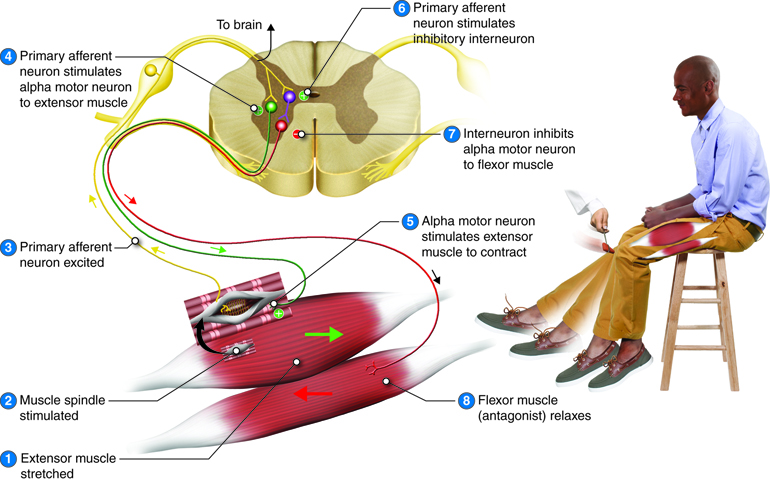
- Testing Reflexes. The knee-jerk reflex or patellar reflex (Figure 16.8)
- Obtain a reflex hammer.
- Ask your classmate to sit on a chair or bench with feet dangling.
- Firmly tap the patellar tendon as shown in the Figure 16.8.
- Does your friend display a knee jerk response? Why does this happen? Explain. ______
Exercise 4 Coordination and Gait Exams
Required Materials
- Your classmates
Procedure
Where you see instructions, ask your “patient” or classmate to follow these. Record what you did and what you observed.
- Testing Lateral Cerebellum Function. Use the tremor check test.
- Ask your classmate to extend the arms in front and hold this position.
- Carefully watch how stable this hold is. Do you see any tremors (shaking) in any part of the arm/upper limb? Record your observations here. Explain what this means for lateral cerebellum function? _________
- Testing of Posture and Gait.
- Ask your classmate to hop on one foot to assess the ability to maintain balance and posture during movement. What do you observe? Explain what this means.______________
- Ask your classmate to walk normally for a distance away from you, and then turn and return to the starting position.
- Watch for abnormal placement of the feet and the movement of the arms relative to the movement. Record your observations. Explain what they mean._________
- Ask your classmate to place the heel of one foot against the toe of the other foot and walks in a straight line in that manner (tandem gait). What do you observe? What does this mean?__________
- Ask your classmate to walk only on the heels. What do you observe? Explain what this means.__________
- Ask your classmate to only walk on the toes. What do you observe? What does this mean? Explain. ________
Post-laboratory Questions
1.The corner of the eye next to the nose is called the ________________________________ and it possesses a fleshy elevation called the _________________________________________.
2. Name the three nerves that innervate the extrinsic eye muscles. _________________, ________________, and ________________________________.
3. The X-shaped structure at the base of the brain where visual images cross over to the opposite side of the brain is called the ________________________________________.
4. Which cranial nerve transmits sensory information from the eye? ________________________________
5. Losing memories of events of the past is called ___________ _________.
6. Loss of the ability to produce speech is _________ ________ and can be caused by damage to ________ area of the brain.
7. Recognizing numbers or letters written on the palm of the hand with a dull pointer is called __________.
8. Registering pain in a part of the body other than the actual source is called __________ __________.
9. Assessing balance by asking the patient to stand up with feet together and close their eyes is the ________ test.
10. A positive sign of _________ is displayed by extension or the toes at the plantar surface of the foot.
