
28 Chapter 28 Development and Inheritance
By Aylin Marz
Motivation.
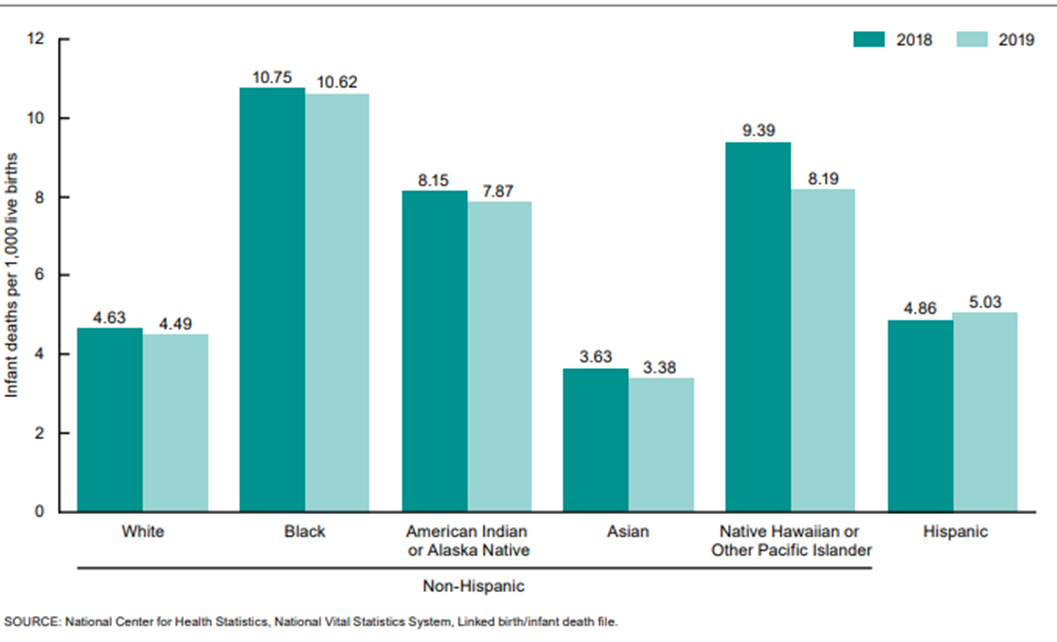
Infant mortality is the death of an infant before his or her first birthday. The infant mortality rate is the number of infant deaths for every 1,000 live births. In addition to giving us key information about maternal and infant health, the infant mortality rate is an important marker of the overall health of a society. In 2020, the infant mortality rate in the United States was 5.4 deaths per 1,000 live births.
Almost 20,000 infants died in the United States in 2020. The five leading causes of infant death in 2020 were:
- Birth defects.
- Preterm birth and low birth weight.
- Sudden infant death syndrome.
- Injuries (e.g., suffocation).
- Maternal pregnancy complications.
Racial and ethnic disparities are abundant and show that African American mothers lose their infants at an alarmingly higher rate than majority/white mothers (Figure 28.1). This is disturbing and we need to better understand how to improve maternal and infant health to fix this problem.
Learning Objectives
Upon completion of the work in this chapter students should be able to:
- Apply knowledge of fertilization and reproductive anatomy to a scenario on IVF success
- Describe the features of embryonic and fetal development using models
- Create models of Punnett squares to determine the outcome of crosses for different types of hereditary diseases
Background.
Fertilization
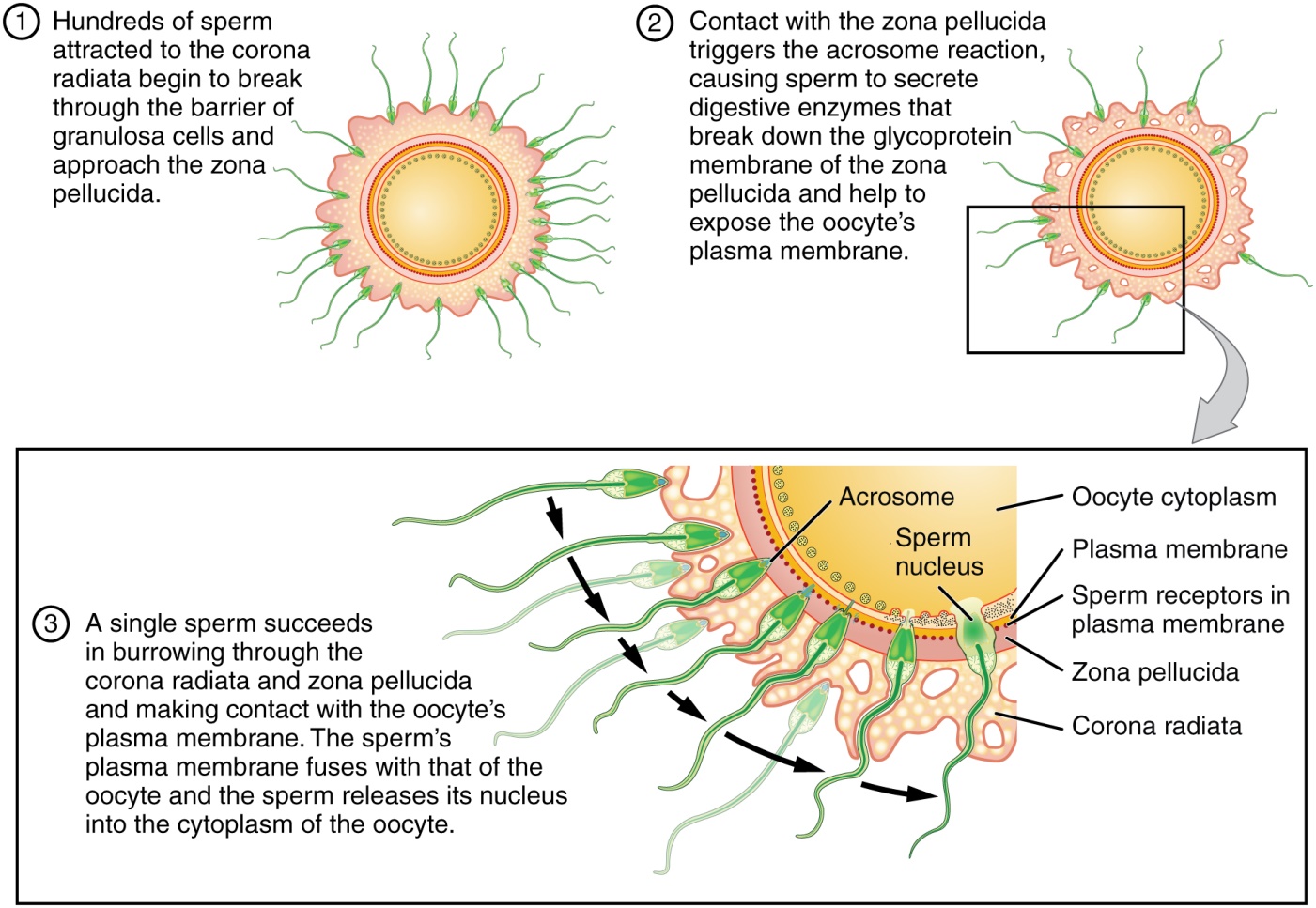
Hundreds of millions of sperm deposited in the vagina travel toward the oocyte, but only a few hundred actually reach it. The number of sperm that reach the oocyte is greatly reduced because of conditions within the female reproductive tract. Many sperm are overcome by the acidity of the vagina, others are blocked by mucus in the cervix, whereas others are attacked by phagocytic leukocytes in the uterus. Those sperm that do survive undergo a change in response to those conditions. They go through the process of capacitation, which improves their motility and alters the membrane surrounding the acrosome, the cap-like structure in the head of a sperm that contains the digestive enzymes needed for it to attach to and penetrate the oocyte.
The oocyte that is released by ovulation is protected by a thick outer layer of granulosa cells known as the corona radiata and by the zona pellucida, a thick glycoprotein membrane that lies just outside the oocyte’s plasma membrane. When capacitated sperm make contact with the oocyte, they release the digestive enzymes in the acrosome (the acrosomal reaction) and are thus able to attach to the oocyte and burrow through to the oocyte’s zona pellucida. One of the sperm will then break through to the oocyte’s plasma membrane and release its haploid nucleus into the oocyte. The oocyte’s membrane structure changes in response (cortical reaction), preventing any further penetration by another sperm and forming a fertilization membrane. Fertilization is complete upon unification of the haploid nuclei of the two gametes, producing a diploid zygote (Figure 28.2).
In vitro fertilization (IVF)
One form of fertility treatment for couples who have trouble conceiving is in vitro fertilization or IVF. In this treatment, the spem and ooctye are fertilized in a “test tube” outside the body. The zygote, after a few divisions, is transplanted into the uterus to allow for development in utero (Figure 28.3).
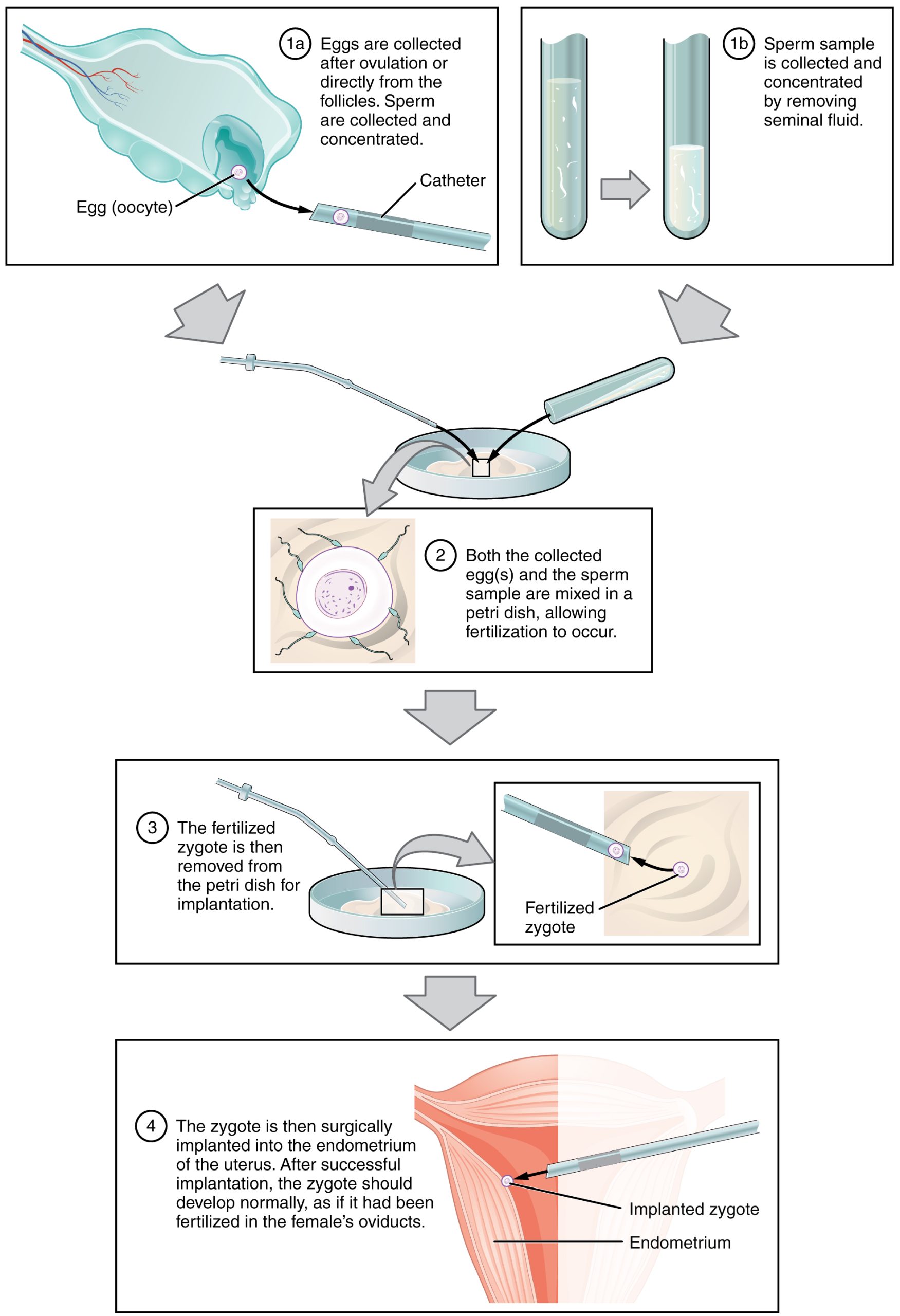
This treatment helps overcome conception issue due to low sperm count, structural difficulties getting sperm and oocyte to meet to fertilize, and structural issues that interfere with the fertilized oocyte to travel down the oviduct to implant into the uterine wall.
Embryonic and Fetal Development
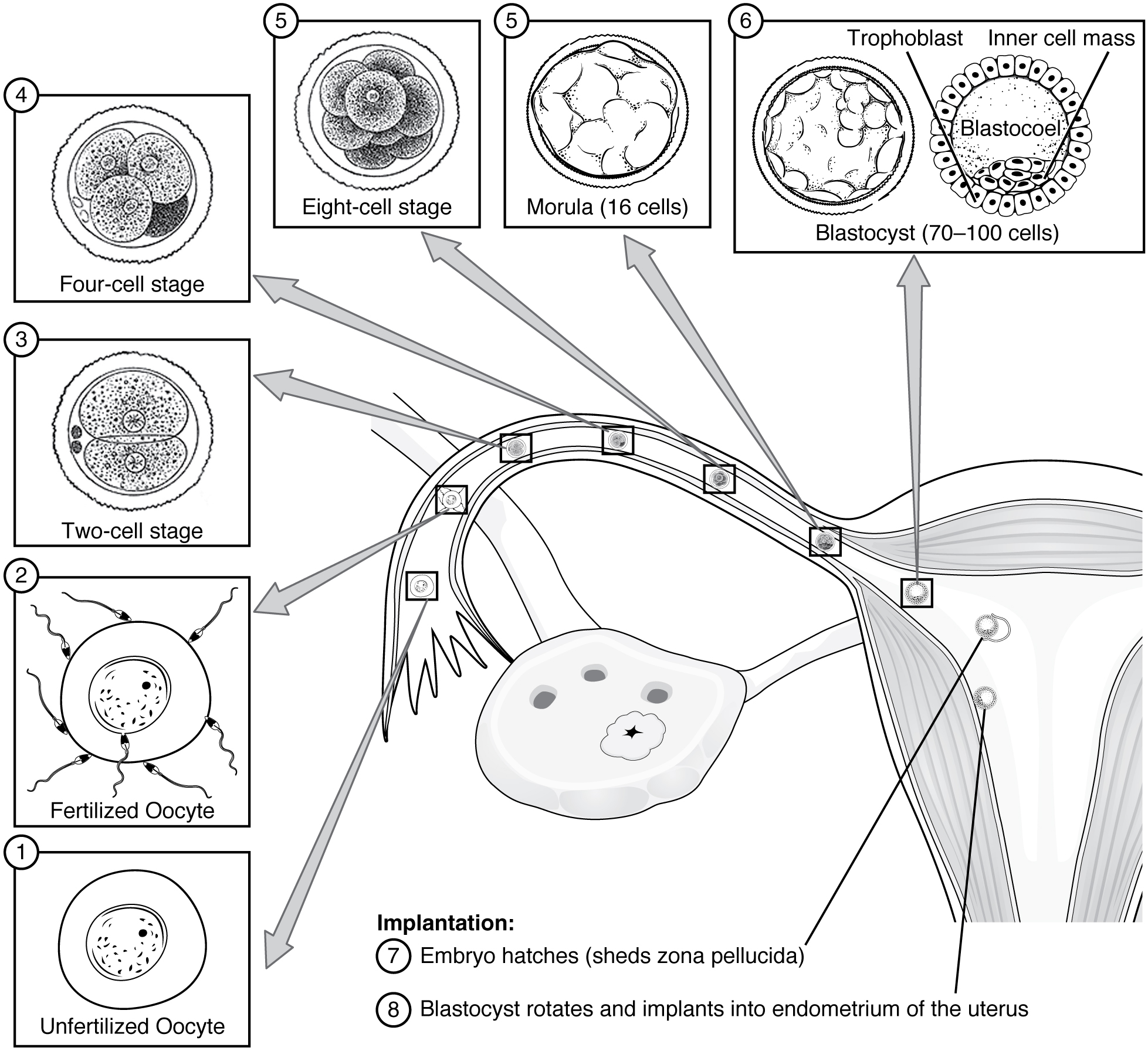
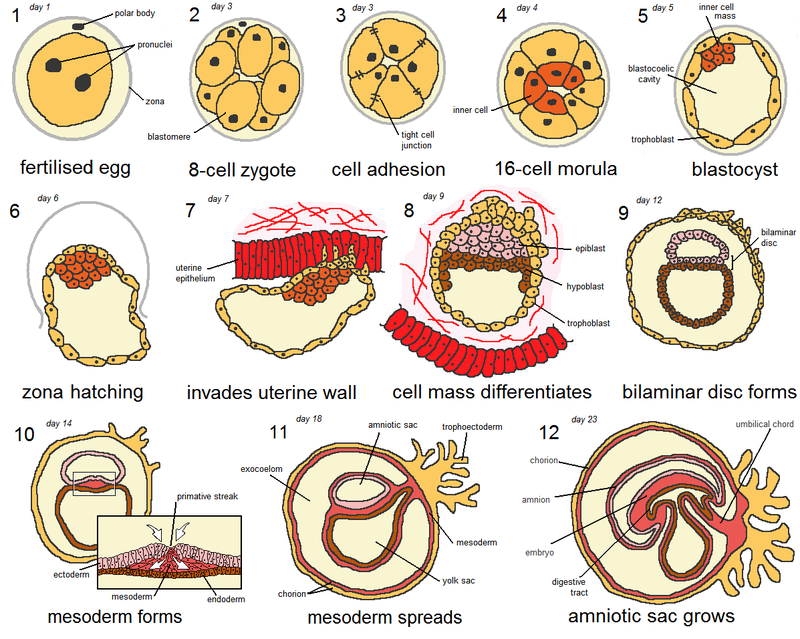
As the zygote travels toward the uterus, it undergoes numerous cleavages in which the number of cells doubles going from one fertilized zygote cell to two-cell, four-cell, eight-cell etc. stages (blastomeres). Upon reaching the uterus, the conceptus has become a tightly packed sphere of cells called the morula, which then forms into a blastocyst consisting of an inner cell mass within a fluid-filled cavity surrounded by trophoblasts. The blastocyst implants in the uterine wall, the trophoblasts fuse to form a syncytiotrophoblast, and the conceptus is enveloped by the endometrium (Figure 28.4).
Four embryonic membranes form to support the growing embryo: the amnion, the yolk sac, the allantois, and the chorion. The chorionic villi of the chorion extend into the endometrium to form the fetal portion of the placenta. The placenta supplies the growing embryo with oxygen and nutrients; it also removes carbon dioxide and other metabolic wastes.
Following implantation, embryonic cells undergo gastrulation, in which they differentiate and separate into an embryonic disc and establish three primary germ layers (the endoderm, mesoderm, and ectoderm). Through the process of embryonic folding, the fetus begins to take shape. Neurulation starts the process of the development of structures of the central nervous system and organogenesis establishes the basic plan for all organ systems. (Figure 28.5)
The fetal period lasts from the ninth week of development until birth. During this period, male and female gonads differentiate. The fetal circulatory system becomes much more specialized and efficient than its embryonic counterpart. It includes three shunts—the ductus venosus, the foramen ovale, and the ductus arteriosus—that enable it to bypass the semifunctional liver and pulmonary circuit until after childbirth. The brain continues to grow and its structures differentiate. Facial features develop, the body elongates, and the skeleton ossifies. In the womb, the developing fetus moves, blinks, practices sucking, and circulates amniotic fluid. The fetus grows from an embryo measuring approximately 3.3 cm (1.3 in) and weighing 7 g (0.25 oz) to an infant measuring approximately 51 cm (20 in) and weighing an average of approximately 3.4 kg (7.5 lbs). Embryonic organ structures that were primitive and nonfunctional develop to the point that the newborn can survive in the outside world (Figure 28.6).

Pregnancy, Labor, Birth and Later Stages. Hormones (especially estrogens, progesterone, and hCG) secreted by the corpus luteum and later by the placenta are responsible for most of the changes experienced during pregnancy. Estrogen maintains the pregnancy, promotes fetal viability, and stimulates tissue growth in the mother and developing fetus. Progesterone prevents new ovarian follicles from developing and suppresses uterine contractility.
Pregnancy weight gain primarily occurs in the breasts and abdominal region. Nausea, heartburn, and frequent urination are common during pregnancy. Maternal blood volume increases by 30 percent during pregnancy and respiratory minute volume increases by 50 percent. The skin may develop stretch marks and melanin production may increase.
Toward the late stages of pregnancy, a drop in progesterone and stretching forces from the fetus lead to increasing uterine irritability and prompt labor. Contractions serve to dilate the cervix and expel the newborn. Delivery of the placenta and associated fetal membranes follows.
The first breath a newborn takes at birth inflates the lungs and dramatically alters the circulatory system, closing the three shunts that directed oxygenated blood away from the lungs and liver during fetal life. Clamping and cutting the umbilical cord collapses the three umbilical blood vessels. The proximal umbilical arteries remain a part of the circulatory system, whereas the distal umbilical arteries and the umbilical vein become fibrotic. The newborn keeps warm by breaking down brown adipose tissue in the process of nonshivering thermogenesis. The first consumption of breast milk or formula floods the newborn’s sterile gastrointestinal tract with beneficial bacteria that eventually establish themselves as the bacterial flora, which aid in digestion.
The lactating mother supplies all the hydration and nutrients that a growing infant needs for the first 4–6 months of life. During pregnancy, the body prepares for lactation by stimulating the growth and development of branching lactiferous ducts and alveoli lined with milk-secreting lactocytes, and by creating colostrum. These functions are attributable to the actions of several hormones, including prolactin. Following childbirth, suckling triggers oxytocin release, which stimulates myoepithelial cells to squeeze milk from alveoli. Breast milk then drains toward the nipple pores to be consumed by the infant. Colostrum, the milk produced in the first postpartum days, provides immunoglobulins that increase the newborn’s immune defenses. Colostrum, transitional milk, and mature breast milk are ideally suited to each stage of the newborn’s development, and breastfeeding helps the newborn’s digestive system expel meconium and clear bilirubin. Mature milk changes from the beginning to the end of a feeding. Foremilk quenches the infant’s thirst, whereas hindmilk satisfies the infant’s appetite.
Patterns of Inheritance. There are two aspects to a person’s genetic makeup. Their genotype refers to the genetic makeup of the chromosomes found in all their cells and the alleles that are passed down from their parents. Their phenotype is the expression of that genotype, based on the interaction of the paired alleles, as well as how environmental conditions affect that expression.
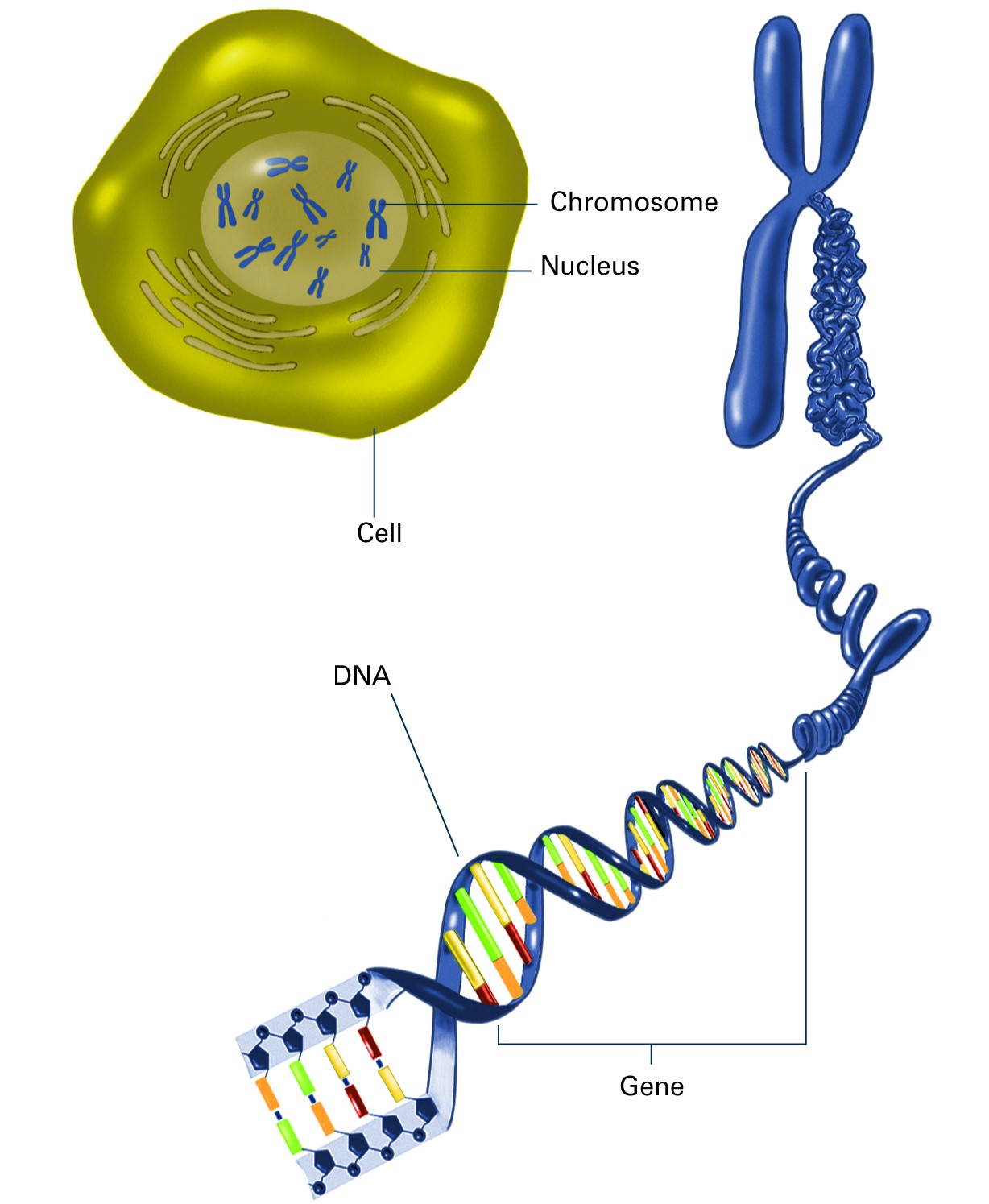
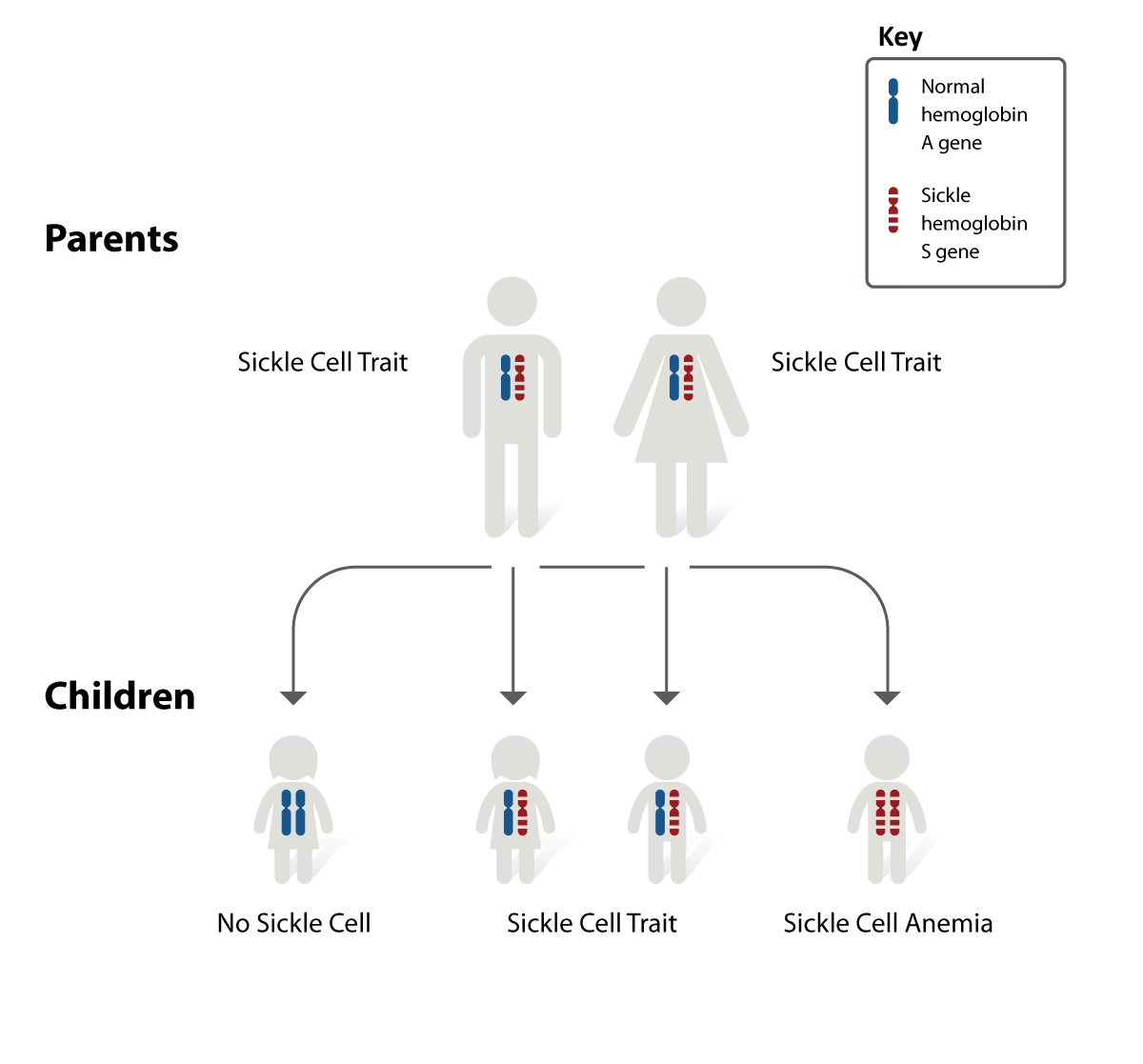
We inherit one copy of a gene from our mother and the other from our father; as genes come in pairs on diploid chromosomes. Each gamete, egg or sperm, has one copy of each gene type. Variants of genes are called alleles. We have a pair of alleles for each trait. Some alleles are dominant over others that are recessive. The dominant allele is expressed or observed if one dominant and one recessive allele are present. For example, for sickle cell anemia the allele HbS is recessive to the normal allele HbA. In order to have sickle cell disease we have to inherit an HbS allele from each parent (Figure 28.8)
Human genetics focuses on identifying different alleles and understanding how they express themselves. Medical researchers are especially interested in the identification of inheritance patterns for genetic disorders, which provides the means to estimate the risk that a given couple’s offspring will inherit a genetic disease or disorder. Patterns of inheritance in humans include autosomal dominance and recessiveness, X-linked dominance and recessiveness, incomplete dominance, codominance, and lethality. A change in the nucleotide sequence of DNA, which may or may not manifest in a phenotype (observed characteristic), is called a mutation.
Pre-Laboratory Questions
- What is IVF?
- At what week of pregnancy do we switch the terminology from embryo to fetus?
- How many alleles of each gene do you have in a diploid cell? In a haploid sperm or egg cell?
Exercises
- Exercise 1 In vitro fertilization (IVF)
- Exercise 2 Embryonic and fetal development
- Exercise 3 Patterns of Inheritance
Exercise 1 In vitro fertilization (IVF)
Required Materials
- Human Uterus and Ovary Pathology Model
- Male Pelvis with Testicular Pathology Model
- Female Reproductive System Poster
- Male Reproductive System Poster
Procedure
1.Examine the Human Uterus and Ovary Pathology Model. List all the pathologies shown on this model that you think would interfere with fertility. For each, explain which part of the process the disorder would interfere with. In the third column, answer the questions “Would IVF help? Yes or No”. In the fourth column, what IVF fixes to enable fertility.
| Pathology | Interferes with (which process in conception) | Would IVF help? | How does IVF help? |
2.Examine the Male Pelvis with Testicular Pathology Model. List all the pathologies shown on this model that you think would interfere with fertility. For each, explain which part of the process the disorder would interfere with. In the third column, answer the questions “Would IVF help? Yes or No”. In the fourth column, what IVF fixes to enable fertility.
| Pathology | Interferes with (which process in conception) | Would IVF help? | How does IVF help? |
Exercise 2 Embryonic and fetal development
Required Materials
- Pregnancy Series Model (3B Scientific L10)
- Complete Anatomy 2022 App by 3D4Medical. Activated by the QR code on the pregnancy series model.
Procedure
- Download the Complete Anatomy 2022 App by 3D4Medical. Activate the app by using the QR code on the Pregnancy Series Model (3B Scientific L10). https://www.youtube.com/watch?v=5sAtUWAn458
- Using the app and other resources available to you examine the 8 models that show the following stages of development / conditions. For each stage / condition, list the main features:
- 1st Month Embryo:
- 2nd Month Embryo:
- 3rd Month Embryo:
- 4th Month Fetus (Transverse Lie):
- 5th Month Fetus (Breech Position):
- 5th Month Fetus (Transverse Lie):
- 5th Month Twin Fetuses (Normal Position):
- 7th Month Fetus:
Exercise 3 Patterns of inheritance
Required Materials
- Wooden sticks
- Marker pens
- Construction paper
Procedure
- In Figure 28.8 we saw an example of how a recessive disease is inherited. We see the potential outcome for children if both parents are carriers (have one copy of the disease allele). In recessive inheritance, you have to have both copies of the recessive allele to have the disease.
- In this exercise, we are going to work with the inheritance of another gene called BRCA1. A mutation in this gene (or an allele of it) increases risk of developing breast cancer. The inheritance of this alelle is dominant.
- Using the wooden sticks, set up the chromosomes of two parents both of whom have one copy of the BRCA1 mutant allele. Use red color for BRCA1 mutant and blue color for normal alleles.
- Place four different construction paper pages onto your desk.
- Work out all possible combinations of alleles that a child of these parents can inherit.
- For each allele combination, indicate whether the child will be at higher risk of developing breast cancer or not. Write down this expected outcome on the paper together with the allele combinations shown with the colorful sticks.
- Take a picture of each of the four scenarios and insert these photos below.

Post-laboratory Questions
- In Exercise 1, would IVF help if a woman had uterine fibroid tumors that interfered with implantation? Explain.
- In Exercise 2, you labeled the main features of embryonic and fetal stages of development. What are the most obvious differences between a 4 month fetus and 7 month fetus?
- In Exercise 3, you worked with a dominant inheritance allele. How is this different than an allele that is inherited in recessive manner. Compare your data to the sickle cell example in Figure 28.8 to help answer this question.
